The human skull contains the following components
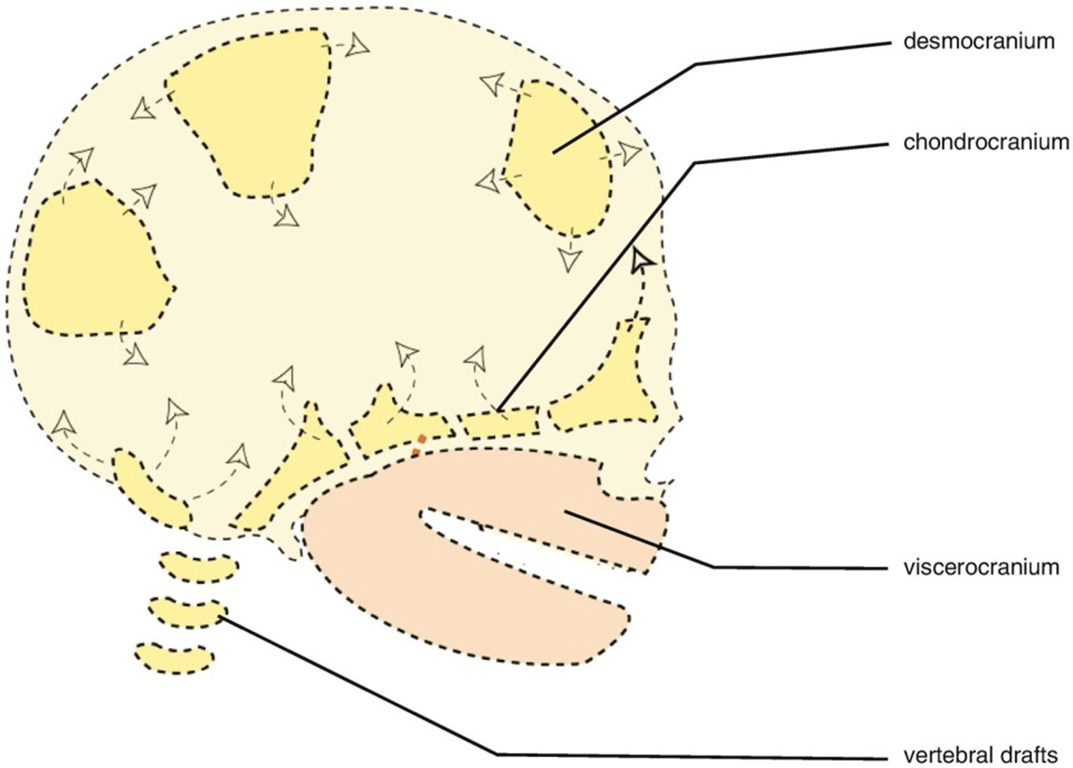
- Neurocranium
- Desmocranuim
- the membranous neurocranium
- Arises from
- neural crest cells
- paraxial mesoderm
- Forms flat bones of the skull
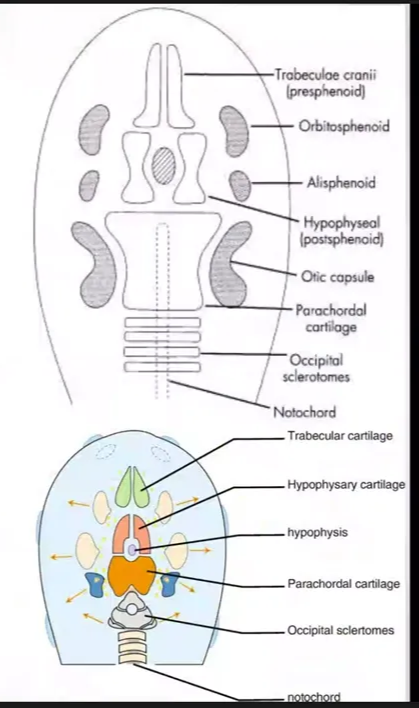
- Chondrocranium
- the cartilaginous neurocranium
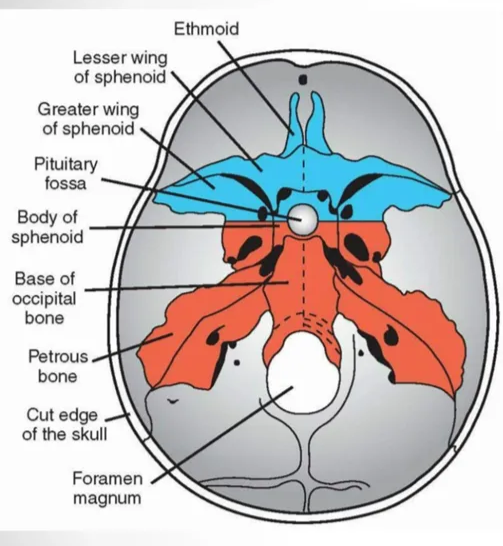
- Forms the majority of the skull base
- Form by
- Arises from
- Neural crest cells
- Cartilage lie cranial to the notochord (hence Prechordal)
- Made up of
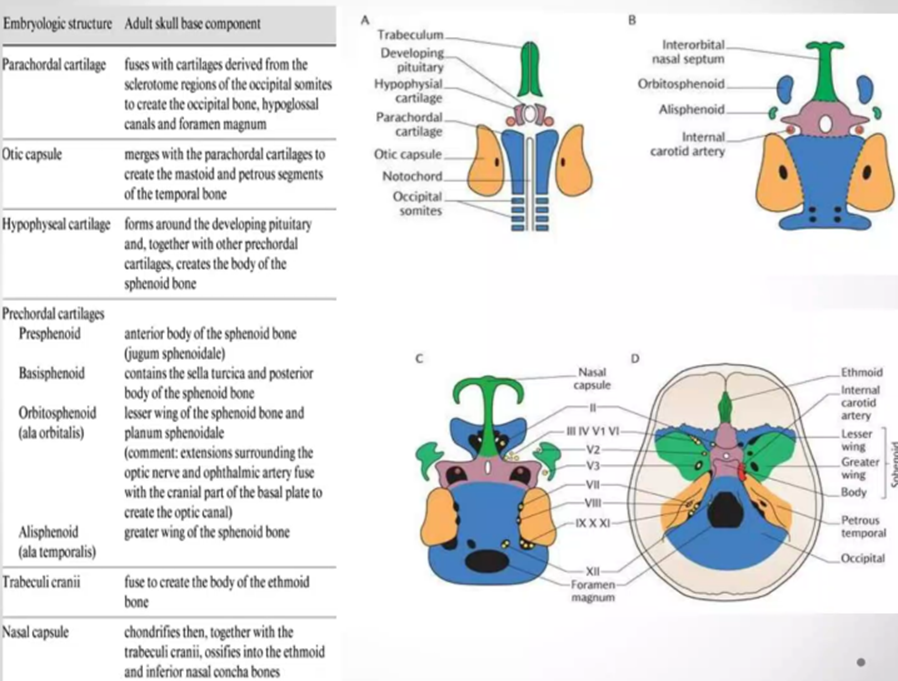
- Trabeculi cranii
- Fuse to create the body of the ethmoid bone
- Nasal capsule
- Chondrifies then together with the trabeculi cranii ossifies into the ethmoid and inferior nasal concha bones
- Otic capsule
- Merges with parachordal cartilages to create the mastoid and petrous segments of the temporal bone
- Presphenoid
- anterior body of the sphenoid bone (jugum sphenoidale)
- Basisphenoid
- Contains the sella turcica and posterior body of the sphenoid bone
- Orbitosphenoid (ala orbitalis)
- Lesser wing of the sphenoid bone and planum sphenoidale
- Extension surrounding the optic nerve and opthalmic artery fuse with the cranial part of the basal plate to create the optic canal
- Alisphenoid (ala temporalis)
- Greater wing of the sphenoid bone
- Forms around the developing pituitary and together with other prechordal cartilages creates the body of the sphenoid bone
- Arises from
- Occipital sclerotomes
- Paraxial mesoderm
- Cartilage lie around the notochord
- Fuses with cartilages derived from the sclerotome regions of the occipital somites to create the occipital bone, hypoglossal canals and foramen magnum
Prechordal Chondrocranium
Hypophyseal cartilage
Parachordal/chordal Chondrocranium
- Viscerocranium
- facial skeleton
Normal Skull growth
- Marked growth of the cranium over first two years of life
- two thirds of which is complete by the age of 2 years.
- Postnatal growth of the calvaria proceeds
- during the first 2 to 3 years of life
- Very rapidly growth
- Cranial growth proceeds primarily through the outward displacement of cranial bones at the sutural margins to accommodate the expanding intracranial volume
- Between 3rd and 7th year of life
- Slow growth
- Cranial growth proceeds primarily through the outward displacement of cranial bones at the sutural margins to accommodate the expanding intracranial volume
- Beyond 7 years
- Most cranial growth occurs by resorption of bone at the inner table and apposition of bone at the outer table
- Though some sutures remain patent until the third decade and beyond
- It is then unable to accommodate significant increases in intracranial volume without potentially dire consequences
1st stage
2nd stage
3rd stage
By early adulthood, the skull has essentially assumed Monro and Kellie’s rigid container, becoming relatively fixed and inelastic.
- Bone growth
- bone growth at the edge of bone while brain expand the sutures
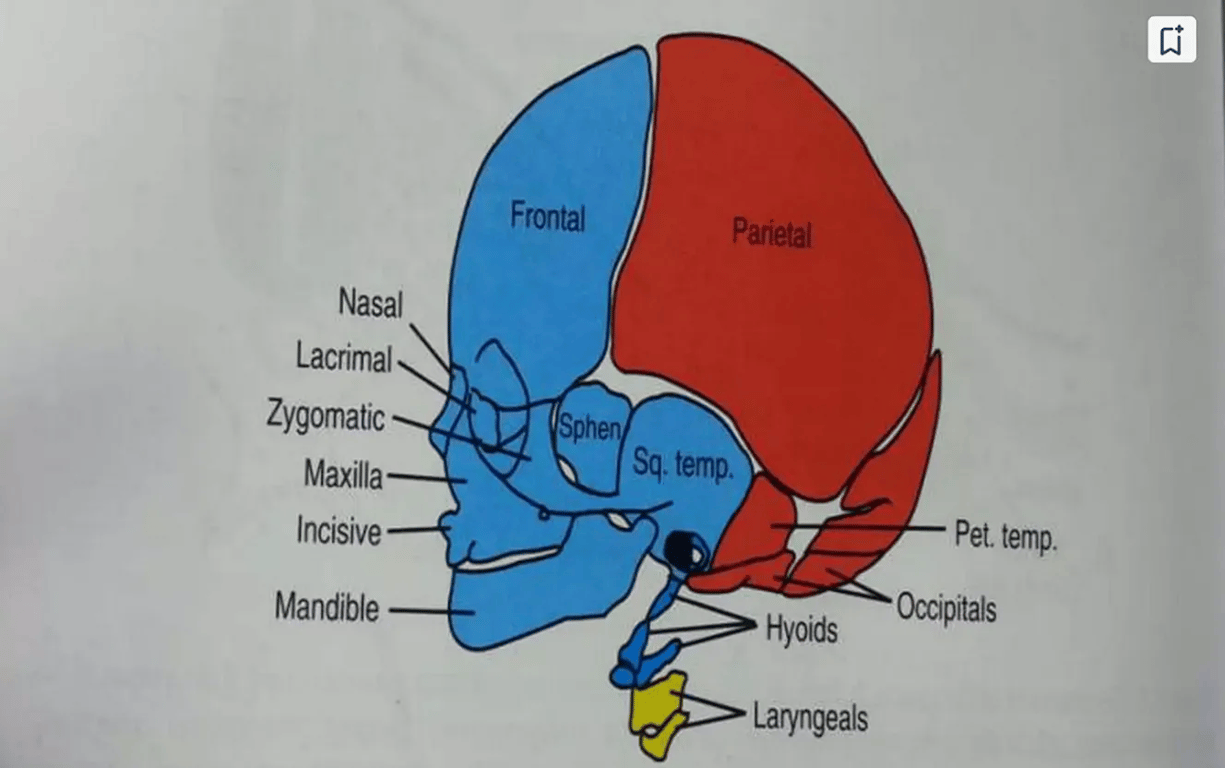
- Heterogenous origin of the calvarial bones
- Frontal bone: neural crest
- Parietal bone: mesoderm lineage
- Age at suture closure
- Posterior: 1-3 months
- Triangle shaped between sagittal and lambdoid sutures
- metopic: 3-9 months
- Only true fusion while others just fibrosis
- Sphenoid (anterolateral): 6 months
- Bilateral; between sphenoid, temporal, parietal, and frontal bones
- Mastoid (posterolateral): 6-18 months
- Bilateral; between temporal, occipital, and parietal bones
- Anterior fontanelle: 18-24 months
- Diamond shaped; between coronal and sagittal sutures (i.e., both frontal and parietal bones)
- sphenosquamosal: 6-10 years
- sphenofrontal: 15 years
- occipitomastoid: 16 years
- sagittal: 22 years
- coronal: 24 years
- lambdoid: 26 years
- squamosal: 60 years
- The amount of bone deposited at the cranial vault suture is related to the strains that influence it, and brain growth is the main driver for the strain
- Skull growth can affect facial bone growth
- Skull growth is triggered by brain growth and CSF pulse pressure
- the outer layer of the cranial dura is the inner periosteal layer of the osseous cranial vault
- Therefore, both the size and morphology of the inner surface of the skull is determined by the dura, which itself is determined by the size and form of the brain
- Ossification of craniofacial bone
- Ossification is centrifugal to create conjunctive boundaries between bone parts.
- These junctions are synfibroses or cranial sutures which allow the passive and functional secondary growth of the bones controlled by the neighboring structures (brain, eyeball, muscular tension, nasal ventilatory flow...).
- The ossification of craniofacial bones has two origins:
- Endochondral
- The base of the skull develops as an enchondral ossification, starting from the cartilaginous base.
- Its growth is independent, or primary, determined genetically and under hormonal control.
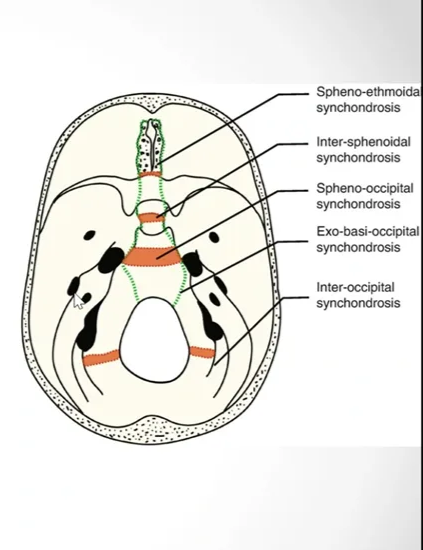
- The borders between the bony parts of the base of the skull are synchondroses which are areas of growth by endochondral ossification whose structure is comparable to that of the epiphyses of the long bones. They have a bilateral growth area or mirrored "dual action epiphysis".
- Inter-sphenoidal synchondrosis - perinatal fusion
- Spheno-ethmoidal synchondrosis - Juvenile/adolescence fusion
- Spheno-occipital synchondrosis - 20yrs fusion
- Principal growth cartilage of the basicranium.
- The sphenooccipital synchondrosis provides a pressure adapted bone growth mechanism.
- This is because the cranial base supports the weight of the brain and face that bears down on the synchondrosis in the midline of cranial base.
- Exo-basi-occipital synchondrosis
- Intra-occipital synchondrosis - Fuses 3-5 years
- Membranous.
- The calvarium and many bones of the facial skeleton are from membranous ossification.
Specific bone growth
Normal foramen magnum growth
- Usually small at birth, the foramen magnum remains small, particularly in the transverse diameter. Growth of the skull is particularly robust and important in the first 18 months of life with achondroplastic patients growing significantly less rapidly
- There is very little difference in the actual size of the foramen between symptomatic and asymptomatic patients; the average adult foramen in patients is the size of the average normal newborn in the transverse diameter and the size of the average 2-year-old in the sagittal diameter
Occipital bone embryonal origin
- The occipital bone has a double origin:
- Endochondral for its basilar part surrounding the foramen magnum
- Membranous for its squamous (flat) part.
 Made with Bullet
Made with Bullet