General
- Composed of 2 distinct but complementary system
- Dorsal subpathway
- Function
- Voluntary, goal-directed allocation of attention towards specific locations or features
- Formed by
- Dorsal fronto-parietal areas, including the
- Dorsolateral prefrontal cortex
- Frontal eye field
- Superior parietal lobule
- Interconnected by layer I of the SLF
- Dorsal attention network is more bilateralized
- Ventral subpathway
- Function
- Reorientation of attention towards unexpected, but behaviorally relevant stimuli
- Formed by
- Inferior frontal gyrus,
- Dorsolateral prefrontal cortex
- Inferior parietal lobule extending to the posterior temporal cortex;
- Interconnected by the layer III of the SLF
- Ventral attention network is right-lateralised
- Communication between ventral and dorsal subpathway
- SLF II that has cortical projections in both networks
- Would play a central role in maintaining functional exchange between them
- IFOF (some parts of it)
- Projects to cortical areas that are involved in spatial awareness
- From
- Posterior DLPFC
- IFOF IV
- Ventrolateral prefrontal
- IFOF III
- Posterior pareital cortex
- Superior parietal lobule
- Angular gyrus
- Breakdown of the right IFOF
- Spatial neglect
Neglect syndrome
Theories
Allocation (attentional or intentional) deficit theory
- Attention: Means by which organisms select stimuli
- Intention: Means by which organisms select and prepare for actions
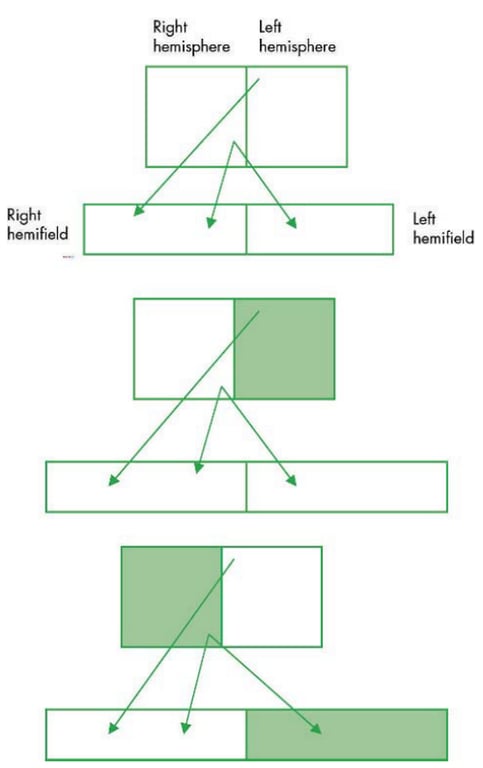
- Each hemisphere mediates attention as well as intention, in and toward the contralateral side of space.
- Neglect is almost always for the left hemifield.
- Left hemisphere monitoring the right hemispace
Right hemisphere monitors both hemispaces. - Left hemisphere lesion does not affect right hemisphere → no hemispace loss
- Right Hemisphere lesion, Left hemisphere still functioning → Right hemispace is still being picked, Left hemispace is neglected
Cognitive theory
- Reflexive form of orienting (bottom-up)
- Automatically evoked by salient stimuli
- Internally controlled form of orienting (top-down)
- Voluntary control
- Spatial neglect
- Is thought to be due primarily to a deficit in bottom up or reflexive orienting
- Stimuli do not automatically attract attention when they are presented in the contralesional side of space.
- This deficit can be overcome to some extent when cues are provided that help patients voluntarily redirect attention to the contralesional portion of space.
- Representational neglect
- May be an example of a failure in top-down processing.
Attention bias theories
- Balance of attention
- Each hemisphere forms a balance of attention between one another → A contralateral orienting deficit disrupts the attentional balance between the two hemispheres → disinhibition of the uninjured hemisphere induced by injury to the opposite hemisphere → manifests as an orienting or attentional bias to the ipsilateral side of space.
- This bias has also been described as attentional capture, or hyperattention.
- Eg: some patients with neglect might more rapidly detect and respond to ipsilesional stimuli that do normal subjects
- Right-hemisphere lesions induce bilateral but asymmetrical inattention, and asymmetrical attention to hemispace induces an ipsilateral attentional bias
- Patients with neglect cannot disengage their attention from ipsilateral stimuli
Unilateral neglect
- An acquired disorder that affects an individual's ability to be aware of or respond to stimuli on the side contralateral to a lesion.
- Disorder cannot be attributed to elementary sensory or motor deficits
- Most resolve over time
- Hemispace
- Not always the midline, rather it is a dynamic construct that is defined by the position of the eyes, head and trunk → when eyes and head moves the hemispaces changes
- Although neglect can occur following lesions of either the left or the right hemisphere, its frequency of occurrence and severity are greater following right- than left-hemisphere dysfunction
- Persistent right-sided neglect is unusual, and when present it should raise the suspicion of bilateral lesions.
- Classification by
- Type
- A failure to detect stimuli presented on the side contralateral to a central nervous system lesion
- Not due to a sensory disturbance but rather to a disruption of the mechanisms responsible for attending to the contralateral side of space
- Manifestation
- Inattention or unawareness of contralateral stimuli
- Patients with sensory neglect or inattention might be unaware of visual, tactile, or auditory stimuli presented to the contralesional side.
- If have bilateral inattention, the contralesional inattention is usually more severe than the ipsilesional inattention.
- Extinction to double simultaneous stimulation
- A less severe form of sensory neglect
- Able to detect stimuli if given it separately in each half of the hemispace but when two stimuli are presented simultaneously to each hemispace (one to each side of the body, to each ear, or to each visual field), patients can only detect one.
- Extinction can also occur when two stimuli are presented on one side of the body or in one visual field.
- The more contralateral of the two stimuli that the patient might not perceive.
- Multimodal extinction is commonly seen during the course of recovery from unilateral inattention.
- Unimodal extinction, in contrast, may occur in the absence of other manifestations of neglect and may be the result of different neuropathological mechanisms
- A failure to respond appropriately to stimuli in the contralateral side of space
- In the absence of
- Weakness and
- Sensory deficit or inattention
- Affects: head and eyes, limbs
- Testing of the contralateral limbs is often impossible owing to the co-occurrence of hemiparesis
- In the acute phase, patients may show a marked deviation of the head, eyes, and trunk to the ipsilesional side.
- Motor bias can also be seen during examination of eye movements, with scanning saccades restricted to the ipsilateral side of space, even though patients may be capable of making full extraocular movements to command
- Manifestation
- Akinesia
- A failure to initiate movements.
- Affects arm, neck, or eyes.
- Frequently have bilateral symptoms but the contralesional limb is more affected
- Contralesional
- Cannot move the contralesional arm
- Cannot turn the head or eyes toward contralesional hemispace.
- Associated with a motor bias, such that the patient's eyes and head might deviate toward ipsilateral hemispace.
- Also, when asked to point straight ahead with their ipsilesional arm with eyes closed, patients with a directional akinesia might point toward ipsilateral hemispace
- Hypokinesia
- A delay in the initiation of a movement,
- Even when the stimuli are presented on the normal (ipsilesional) side.
- Delays in initiation can be seen bilaterally but is more severe in the contralesional forelimb.
- Can also be directional (movements toward contralesional hemispace) or hemispatial (movements in contralesional hemispace).
- Motor impersistence
- A failure to sustain a movement or posture.
- This impersistence can be for movements that are directed toward or in contralateral space (e.g., sustained leftward gaze).
- Motor extinction
- A failure to move or maintain movement of the contralateral limb when the ipsilateral limb is moved simultaneously.
- Like sensory extinction, motor extinction often occurs during the course of recovery and represents a mild form of motor neglect.
- Location
- Personal: personal neglect
- Attentional disturbances for the contralateral side of their body.
- Fail to discriminate the position of their contralateral limb or neglect to use objects such as a comb or razor on the contralateral side of their own body.
- Associated with representational neglect at the contralateral side of their body
- Eg: When asked to identify pictures of the left or right hand seen from the palm or from the back, they perform poorly, which suggests that they are unable to match perceptual information to body representations
- Extrapersonal (hemispace neglect)
- Peripersonal: close extrapersonal
- Show attentional disturbances within reaching or grasping space
- Test
- Perform poorly when line bisection or search tasks are presented 30 to 60 cm away from their body but not when the stimuli are presented further away.
- Far extrapersonal:
- Show attentional disturbance far away
- Frame of reference
- Environmental neglect:
- When attention operates on a global environmental spatial array, independent of the orientation of the patient's body, one side of the environment is ignored
- Viewer-centered neglect:
- When attention operates within segregated figures, as defined by the patient's viewpoint, the portion of the stimulus that is on the contralesional side of the patient might be ignored
- Under most ordinary circumstances, the environmentally centered, object-centered, and viewer-centered frames of reference coincide with each other.
- Object-centered neglect
- When the spatial coordinates intrinsic to an object form the frame of reference within which attention operates (regardless of the position of the object in the environment and its relationship to the viewer), the contralateral portion of this object might be unattended.
- When some patients are asked to imagine a scene or a part of their body, they may fail to report portions on the side opposite to their lesion.
- Although representational neglect is often associated with hemispatial or personal neglect, these disorders might be dissociable. Some patients with neglect might also have difficulty recalling perceived contralateral stimuli
Sensory neglect/inattention/afferent/perceptual neglect.
Motor/intentional/efferent neglect
Space
Representational Neglect
Type of neglect | Manifestations | Sectors of space |
Sensory neglect | Unawareness of contralateral stimuli; allesthesia; extinction | Personal; peripersonal; far extrapersonal |
Motor neglect | Akinesia; hypokinesia; motor impersistence; motor extinction | Personal; peripersonal; far extrapersonal |
Pathophysiology
- Cause by
- Vascular disease
- Thrombotic infarction
- Embolic infarction
- Haemorrhage
- Tumours
- Degenerative diseases.
- Seizure
- Ictal
- Postictal
- Site of damage
- Inferior parietal lobe (most common)
- Directing attention to information that is coded in a spatial framework
- Other
- Frontal cortex,
- Frontal eye fields, are critical for coordinating the motor programs for exploration, scanning, and navigation in space.
- Cingulate gyms,
- Motivational significance of stimuli
- Basal ganglia,
- Thalamus, and reticular formation
- Modulation of the overall level of arousal and vigilance
- Dorsal (parietal) lesions can induce neglect of lower space,
- Ventral lesions might be associated with neglect of upper space
Anatomical substrate | Putative contribution |
Parietal lobe | Orienting of attention, spatial representation |
Prefrontal lobe | Motor intention |
Basal ganglia | Motor control |
Reticular formation, intralaminar thalamic nuclei | Arousal |
Anterior cingulate | Motivation for action |
Posterior cingulate | Stimulus significance |
- Mech
- Sensory neglect/inattention:
- Disruption in the parietal and limbic (posterior cingulate) components of the attentional network
- Motor intentional/neglect:
- Disruption in the prefrontal, basal ganglionic, and limbic (anterior cingulate) components.
- Both sensory and motor neglect/inattention
- Thalamus and reticular formation
Assessment
- Patient interactions with examiner and environment
- Sensory Neglect or Inattention
- Asking the patient to detect the presence and location of
- Auditory stimuli
- While the patient is blindfolded, either making a noise by rubbing or snapping fingers near the patient's left or right ear or not making a noise
- Visual stimuli
- Placing one hand in the patient's left visual field and the other in the right and either moving or not moving the left or right index finger
- Tactile stimuli
- With the patient blindfolded, touching the ipsilateral and contralateral hand in random order or not touching
- Extinction
- Following testing for unilateral inattention, if the patient was able to detect stimuli on the side contralateral to his or her lesion, the examiner should also test for extinction to simultaneous stimulation by intermixing unilateral trials with trials on which two stimuli are presented simultaneously to homologous areas of space or body.
- Personal Neglect
- Patients who are unaware of the contralesional side of their body will often fail to groom or dress that part of their body. Thus, it might be important to observe a patient when he or she grooms and dresses.
- Different commands that require orienting to or awareness of contralateral body parts can also be used to test for personal neglect. For example,
- Patients can be asked to touch their contralateral side with the ipsilateral extremity.
- Patients with neglect may interrupt their movement before the target is reached or may fail to initiate a movement to the contralateral limb.
- Asking patients to match parts of their body with external representations, for example, to touch on their own body the body part pointed out on a model or to point to a body part on a model when it is touched on their own body.
- Patient shown either their own hand versus the examiner's hand and asked whose hand is indicated.
- Patients with personal neglect might claim that their own left hand belongs to the examiner.
- Hemispatial or Unilateral Neglect
- Most standardized tests of spatial neglect consist of visual tasks performed in peripersonal space, but several can also be performed in far extrapersonal space or can be easily adapted to the tactile modality. Despite the surface similarity among these tasks, several investigators have demonstrated that these tasks assess more than a single neuropsychological process, and thus patients with spatial neglect might show dissociations in their performance on these tests. For this reason, a broad-based assessment is needed.
- Moving finger test
- Moving one, other, or both fingers in right and left hemifields and asking the patient which finger has moved.
- In visual extinction, the patient will note either finger moving separately, but will only detect the finger in their right hemifield when presented simultaneously.
- This is due to the ipsilesional stimulus ‘‘extinguishing’’ the contralesional stimulus from awareness.
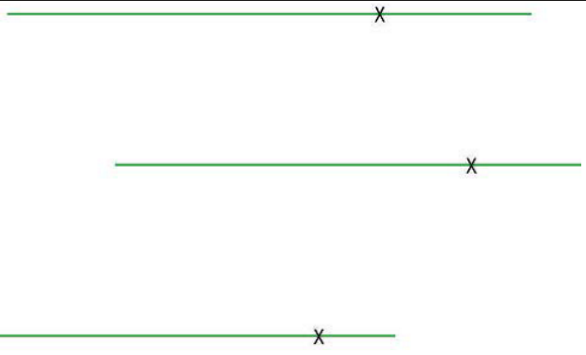
- Line bisection tasks
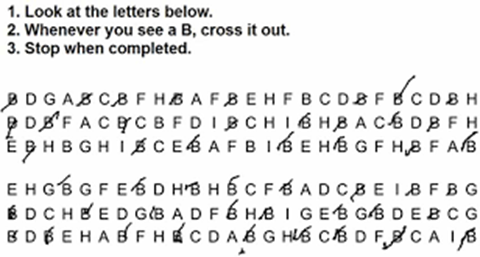
- Letter cancellation tasks
- Reading and writing test
- Reading
- Menu Reading, in which 10 food items, one or two words long, are presented for reading in two columns, and
- Article Reading, in which two paragraphs are presented in a columnar arrangement, similar to a newspaper article
- Writing
- Drawing a clock face
- Imagery task
- No standardized assessment techniques are available to test imagery.
- Asks patient to imagine a familiar scene and to tell the examiner what he or she sees in his or her mind eye.
- If the examiner is not familiar with the scene (such as a patient's home), it is important to get the aid of a person who is able to corroborate the patient's description.
Other associated disorders
- Anosognosia ( a-, "without", νόσος nosos, "disease" and γνῶσις gnōsis, "knowledge)
- Inability to recognise consciously the presence of somatic dysfunction indicative of a disease process.
- Patients with left hemiplegia caused by stroke may be entirely unaware of their deficit.
- It presents acutely after ictus
- Caused by
- Non-dominant parietal lesions (covers both Left and Right Hemispace)
- Most common cause
- May be due to
- Failure of feedback induced by sensory deficits or inattention,
- Deficit in body image (asomatognosia),
- Intentional disorder in which there is a failure to develop an expectation,
- Interhemispheric disconnection such that the left hemisphere confabulates a response
- Regarded more a disorder of attention than of perception.
- Anosodiaphoria
- Partial recovery after Anosognosia (After a few days or week) → starts acknowledge their illness but appear unconcerned about their illness and disabilities or may even joke about their disabilities.
- This aberrant behaviour might be related to emotional disorders associated with right-hemisphere damage or the fact that patients have only a partial awareness of disability
- Other Visuospatial Deficits
- Right-hemisphere lesions
- Deficits in processing of global information → have a bias toward processing of local objects
- More debilitating
- A visual display contains more local than global information. Because patients with right-hemisphere lesions are biased toward local information, it becomes even more difficult for them to move their attention away from local objects in ipsilesional space
- Left hemisphere lesions
- Deficits in processing local information → have a bias toward processing global scenes.
- Allesthesia and Allokinesia
- Allesthesia
- Input deficit
- When stimulated on the contralesional (e.g., left) side and asked where they were stimulated, some patients with neglect indicate that they were stimulated on the ipsilateral (e.g., right) side.
- Although some investigators have proposed that this disorder might be related to a hemispatial and hemibody representational deficit, the cognitive mechanism underlying this disorder is not completely understood.
- Allokinesia
- Output deficit.
- When stimulated on the contralesional side (e.g., left) and asked to move the ipsilesional limb (Right) in the direction of the stimulation, the patient moves in an ipsilesional (e.g., rightward) direction.
- Similarly, when asked to move the stimulated (contralesional) limb, the patient moves the ipsilesional (e.g., right) limb.
- Unlike patients who have allesthesia, patients with allokinesia can correctly localize the position of the stimulus verbally.
- Although allokinesia is often associated with directional or limb akinesia, the mechanisms of this disorder are also incompletely understood.
Treatment
- Inducing illusion of environmental movement by
- Vestibular stimulation (e.g., cold water caloric stimulation) or
- Moving the background can reduce the signs of neglect, but only temporarily.
- Behavioural treatments
- Training patients to orient to the left side of space, having them learn to move the left side of their body
- Having pt wear prism glasses while providing midline training.
- Patching the ipsilesional eye might improve some patients, but others improve with patching of the contralesional eye
- Drugs
- Dopamine agonists have also been reported to improve neglect
- But if a patient's lesion extends into the basal ganglia, this treatment might make their neglect more severe.
 Made with Bullet
Made with Bullet