General
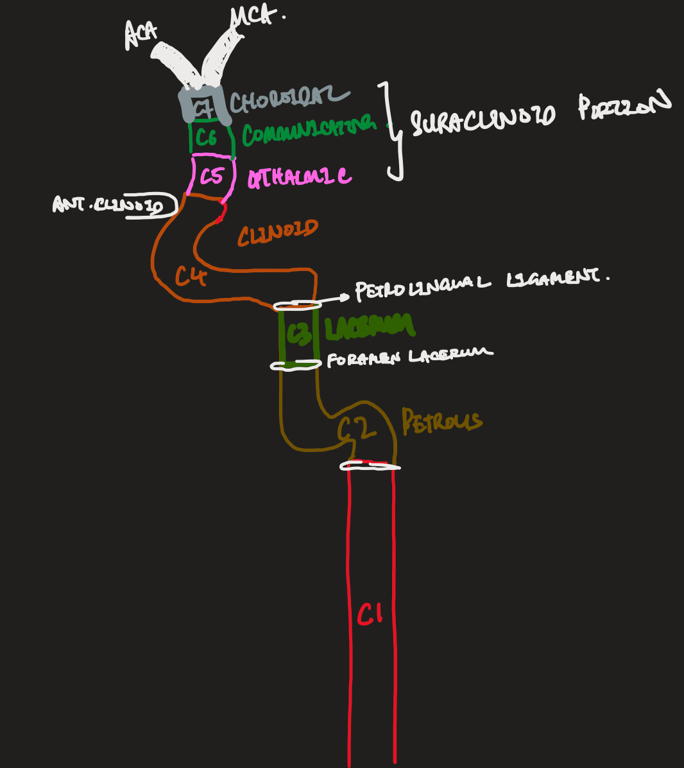
Bouthlier classification of ICA
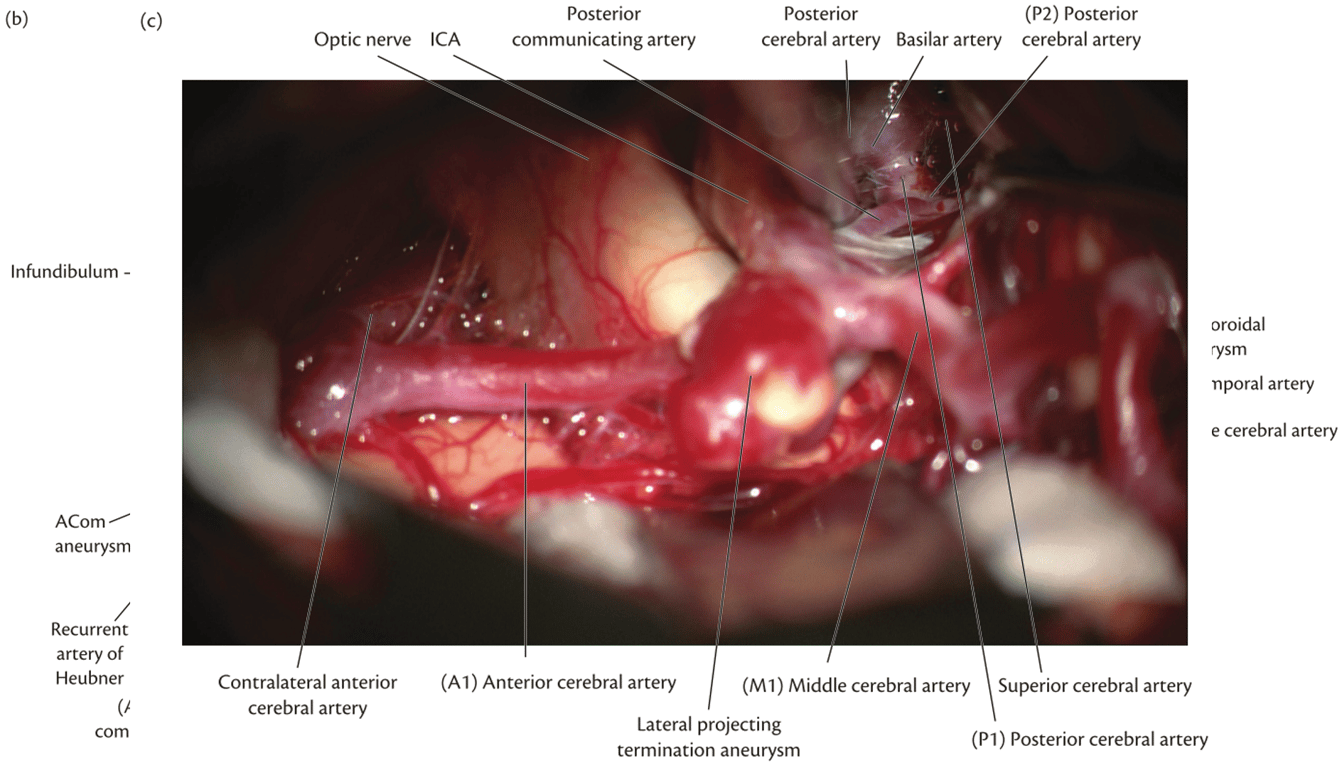
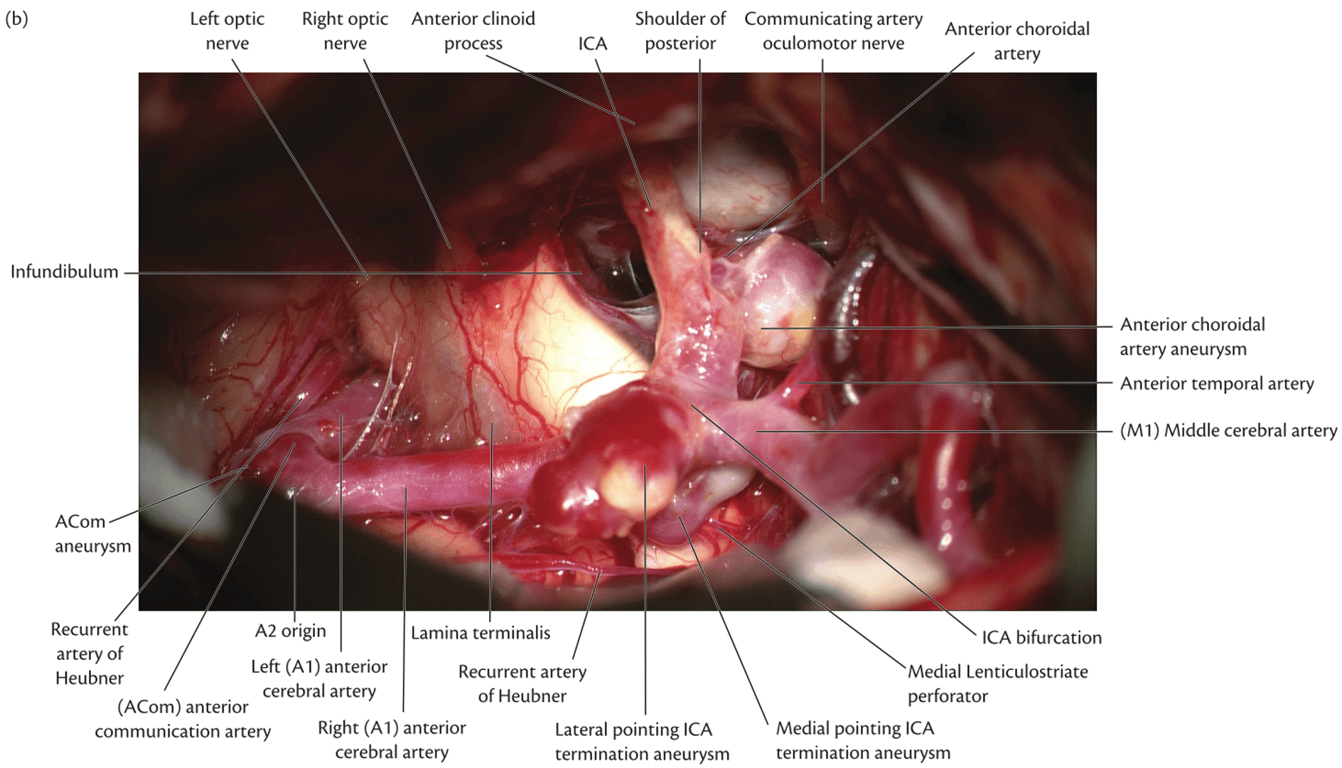
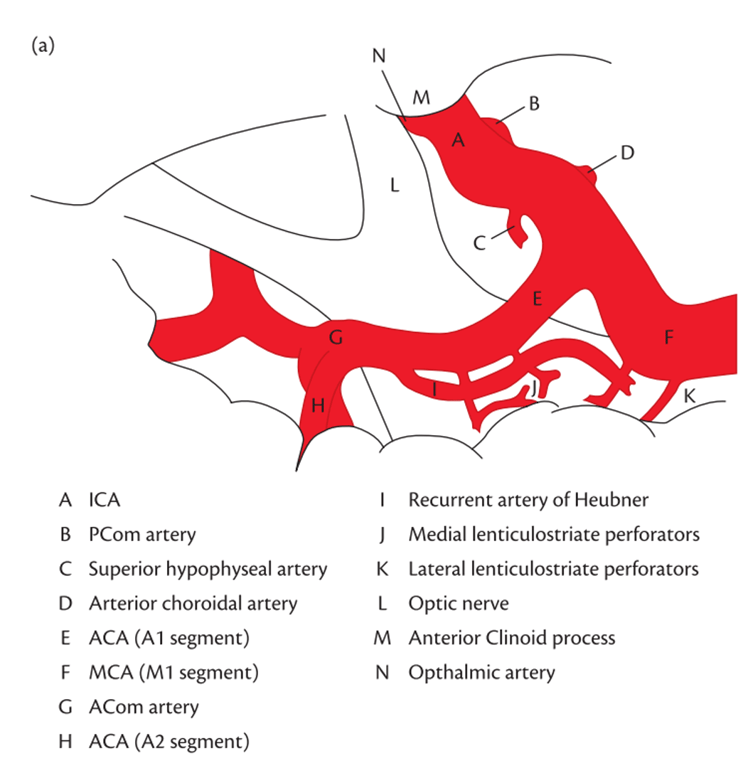
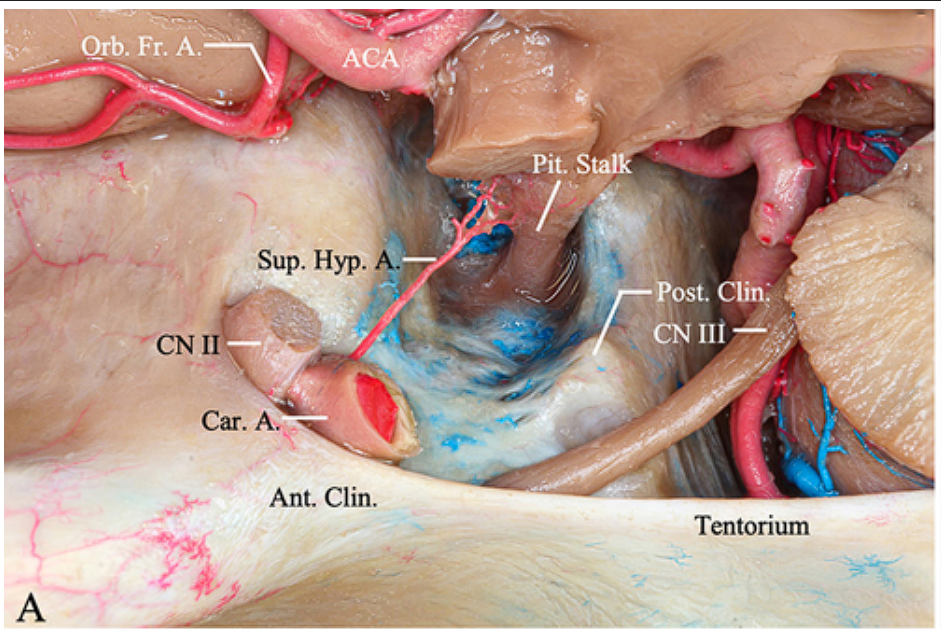
- View of the ICA after sylvian fissure split following pterional craniotomy showing major arterial vessels at base of brain
Cervical C1
- No branches
- Separation: External orifice of carotid canal
Petrous C2
- Caroticotympanic artery
- Embryonic hyoid artery remnant
- Aberrant course can cause a retrotympanic pulsating mass
- Anastomosis with inferior tympanic artery (branch of ascending pharyngeal artery)
- Vidian artery
- Artery of the pterygoid canal
- Travel through vidian canal and foramen laceraum
- Anastomosis with ECA
Separation: Foramen lacerum
Lacerum C3
Intercavernous C4
- ICA enters the posterior part of the cavernous sinus, where it runs forwards.
- ICA is surrounded by sinus endothelium and supported by trabeculae
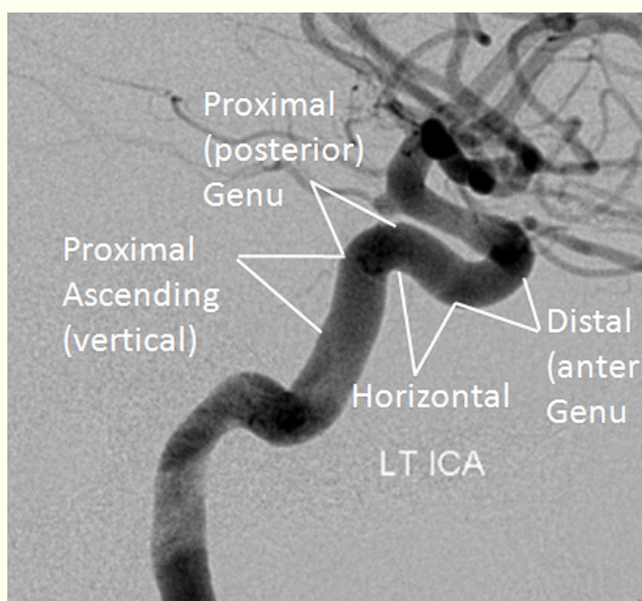
- Carotid siphon: U-shaped section of the ICA, formed from mostly the cavernous portion
Segments
- Ascending Portion
- Posterior Genu
- Horizontal Portion
- Anterior Genu
3 branches
- Meningohypophyseal trunk (largest branch) (A)
- From ascending portion
- Branches
- Dorsal meningeal artery (clival branch): CN6 + part of clivus
- Main branches
- Lateral Tentorial Artery (B)
- Along the lateral edge of the tentorium,
- In hemodynamic balance with
- Petrosquamosal branches (L) of the Middle meningeal Artery AND
- Occipital Artery (O)
- Marginal Tentorial Artery (C) a.k.a. Tentorial artery of Bernasconi and Cassinari along the free edge;
- Inferior Hypophyseal Artery (D), branches into:
- Hypophyseal branches (E)
- Supplying the posterior and parts of anterior pituitary
- Anastomosing with each other
- Inferior Clival Branch (F)
- Descending along the dorsum sella
- It is in hemodynamic balance with the ascending clival braches (K) of the Ascending Pharyngeal
- Lateral Clival artery (G), branching into:
- Lateral Branch of the Lateral Clival artery (H)
- Runs alongside the Superior Petrosal Sinus
- Medial Branch of the Lateral Clival Artery (I)
- Runs alongside the Inferior Petrosal Sinus
- Is in haemodynamic balance with Jugular branches (J) of the Ascending Pharyngeal
- Dorsal meningeal artery (clival branch): CN6 + part of clivus
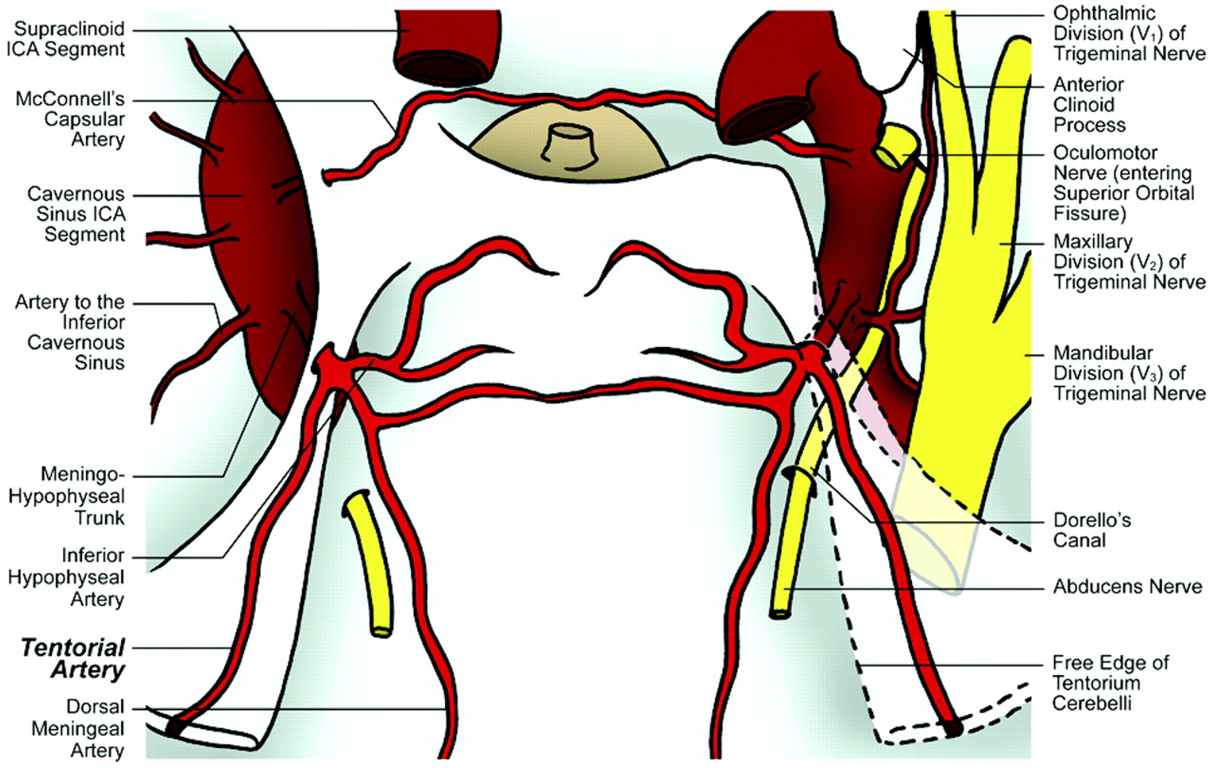
- Inferolateral trunk (Aka: artery of the inferior cavernous sinus)
- From anterior genu
- Anastomosis with
- Maxillary artery ( through artery of foramen rotundum
- MMA + Ophthalmic artery
- Travels/supply to: floor of the middle cranial fossa /cranial nerves of Cavernous sinus
- inferior lateral cavernous sinus wall
- Tentorium (via tentorial branch)
- CN III,IV, VI and Gasserian (trigeminal) ganglion (via Foramen Ovale/spinosum to supply)
- It is in balance with middle and accessory meningeal arteries
I, McConnell's capsular arteries
- Aka
- Medial trunk
- McConnell's capsular arteries
- Supplies
- Sellar region, in particular, to the sella dura mater and the anterior pituitary capsule
- Branches into
- Anterior capsular artery
- Inferior capsular artery
- Courses inferior
- Least constant of the three major branches (30% present) of the intercavernous ICA
Separation: Proximal dural ring
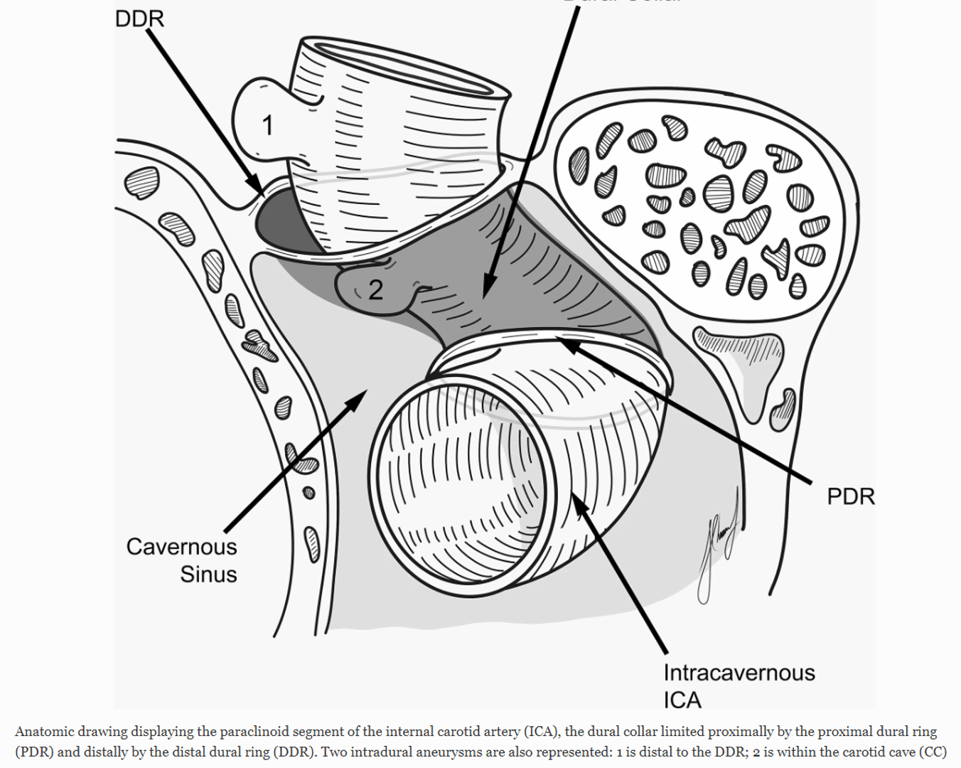
Clinoidal segment
- The clinoidal carotid segment is a transitional segment between the cavernous sinus before the ICA exits through the distal ring and enters the subarachnoid space
- Two rings are fused posteriorly, they are variably separated anteriorly, giving rise to two regions medially and laterally.
- The lateral region may be considered to be extradural and extracavernous.
- On the medial side, the space between a redundant portion of distal dural ring and ICA is termed the carotid cave.
- Although usually extradural, rupture of carotid cave aneurysm extending superiorly out of the cave may result in subarachnoid haemorrhage
- Distal dural ring sits inclined posterior-medially and is continuous medially with the falciform ligament and with the dura overlying the superior-medial aspect of the anterior clinoid process
- Surgically understanding of this region is important as access to proximal aneurysms at or near the origin of the ophthalmic artery will require an anterior clinoidectomy
- Distal ring is not visible radiologically and its location can only be estimated.
- Clinically this region is important as the distal dural ring differentiates aneurysms that cause subarachnoid haemorrhage versus those that cause carotico-cavernous fistulae.
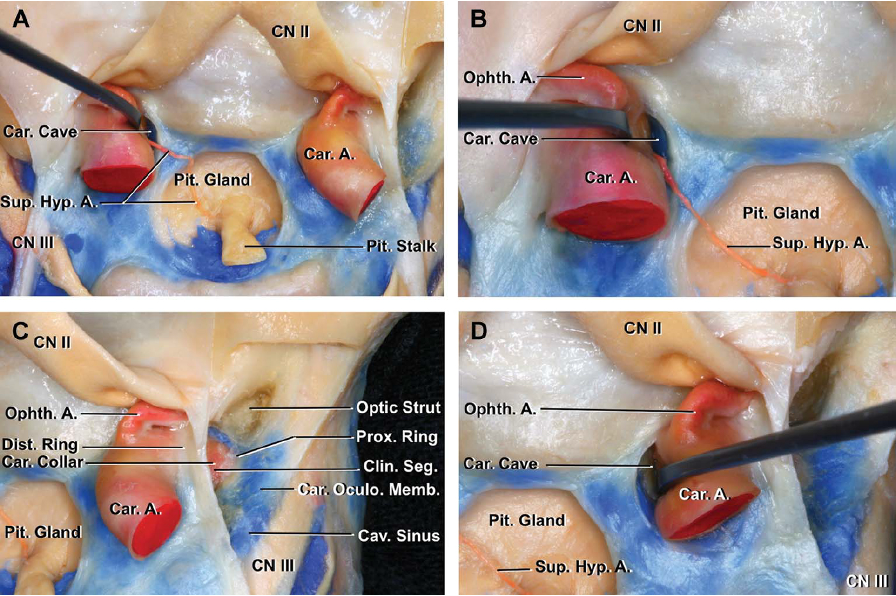
- Anatomical Exposure and Regions
- The optic strut is exposed in the anterior part of the clinoidal triangle.
- The clinoid segment is exposed in the midportion.
- The roof of the cavernous sinus is exposed in the posterior part.
- The posterior bend of the internal carotid artery (ICA) and the origin of the meningohypophyseal trunk are exposed in the infratrochlear triangle.
- Dural Rings and Membranes
- The upper margin of the clinoid segment is surrounded by the upper dural ring.
- The upper dural ring is formed by the dura extending medially from the upper surface of the anterior clinoid.
- The lower dural ring defines the lower margin of the clinoid segment.
- The dura on the lower margin of the anterior clinoid is referred to as the carotidoculomotor membrane.
- The carotidoculomotor membrane separates the lower surface of the anterior clinoid from the upper surface of the oculomotor nerve.
- This membrane extends medially to form the lower dural ring.
- Internal Carotid Artery (ICA) and Branches
- The meningohypophyseal trunk arises near the posterior bend of the ICA.
- The meningohypophyseal trunk gives rise to the tentorial and dorsal meningeal arteries.
- The inferolateral trunk arises from the horizontal segment of the intracavernous carotid.
- Cranial Nerve Pathways
- The abducens nerve passes through Dorello’s canal.
- The abducens nerve passes between the lateral surface of the intracavernous carotid and the medial side of the ophthalmic nerve.
- The inferolateral trunk passes above the abducens nerve.
Separation: Distal dural ring
Ophthalmic segment C5
Ophthalmic artery (Has a bayonet shape- can be used to identify on DSA)
- Origin
- just beyond the distal dural ring
- inferior to the optic nerve and anterior clinoid process
- enters the orbit through the optic foramen.
- 1st intracranial ICA branch
- 0.5% arises from MMA (Meningo-opthalmic artery)
- arising from the middle meningeal artery and entering the orbit through the superior orbital fissure may replace the ophthalmic artery
- Can lead to blindness if MMA is embolized
- Branches
- Ocular branches: Supplies retina, choroid of eye, optic nerve
- Central Retinal artery
- Ciliary artery
- Orbital branches
- Lacrimal artery: Lacrimal gland, conjunctiva
- Recurrent meningeal artery turns backwards through superior orbital fissure to anastomose with MMA
- Muscular artery: extraocular muscle, orbital periosteum
- Extraorbital branches: Extensive anastomosis with ECA for collateral intracranial flow during proximal ICA occlusion
- Supraorbital
- Anterior and posterior Ethmoidal
- Anterior ethmoidal is a landmark for the frontal sinus
- Dorsal Nasal
- Medial frontal
- Palpebral
- Superior trochlear
- Aneurysm arising from the ICA distal to the ophthalmic artery: points upwards towards the optic nerve
Superior hypophyseal artery
- Several small arteries arsing from posterior medial portion of intradural ICA
- Courses under optic nerve
- Supplies
- Pituitary
- Parts
- Ant Pituitary
- Pituitary stalk
- Tuber cinereum
- Anastomosis (forms hypophyseal portal system)
- With contralateral side
- Inferior hypophyseal artery
- Optic nerve and chiasm (inferior surface)
- Aneurysm
- Mimics a pituitary adenoma
- arising here points inferiorly and medially
- Of note, aneurysms within the clinoid, ophthalmic and hypophyseal region are frequently termed ‘paraopthalmic’ aneurysms, reflecting the difficulty in their angiographic localization.
Communicating C6
Posterior communicating artery
- Branches
- 7 perforator evenly distributed along PComA courses superior medially to supply
- Post hypothalamus
- Ant Thalamus
- Sub thalamic
- Post limb of internal capsule
- Course
- arises from the dorsolateral aspect of the ICA, and connects after approximately 1 cm, to the posterior cerebral artery,
- has an entirely cisternal trajectory; however, it is encased in a sleeve of arachnoid membrane
- runs posteromedially below the tuber cinereum above the Sella turcica and oculomotor nerve, close to the dura overlying the posterior clinoid process, before piercing the Lilliquist membrane of the interpeduncular cistern to join the posterior cerebral artery.
- close proximity to the oculomotor nerve- surgical (involving the pupil) third nerve palsy.
- Aneurysm
- Arise from post wall of ICA just distal to PComA origin , and point posteriorly towards CN III
Variant: Present in 50% cases
- Absent (hypoplastic PComA): 30%
- Foetal variant of PCA: 20%
- P1 has a smaller diameter than the PComA and the PCA arises predominantly from the ICA
- Foetal PCA fail to regress
- Occurs 1/3 of hemispheres 25% of people
- danger that if anterior circulation is occluded the occipital lobe will be ischaemic
- Infundibular: 10%
- Looks like an aneurysm but is not
- Funnel shaped dilatation observed at junction between PComA and ICA
- Infundibular has a vessel at the apex of the infundibular "aneurysm"
Normal

Aneurysmal

Infundibular

Images:
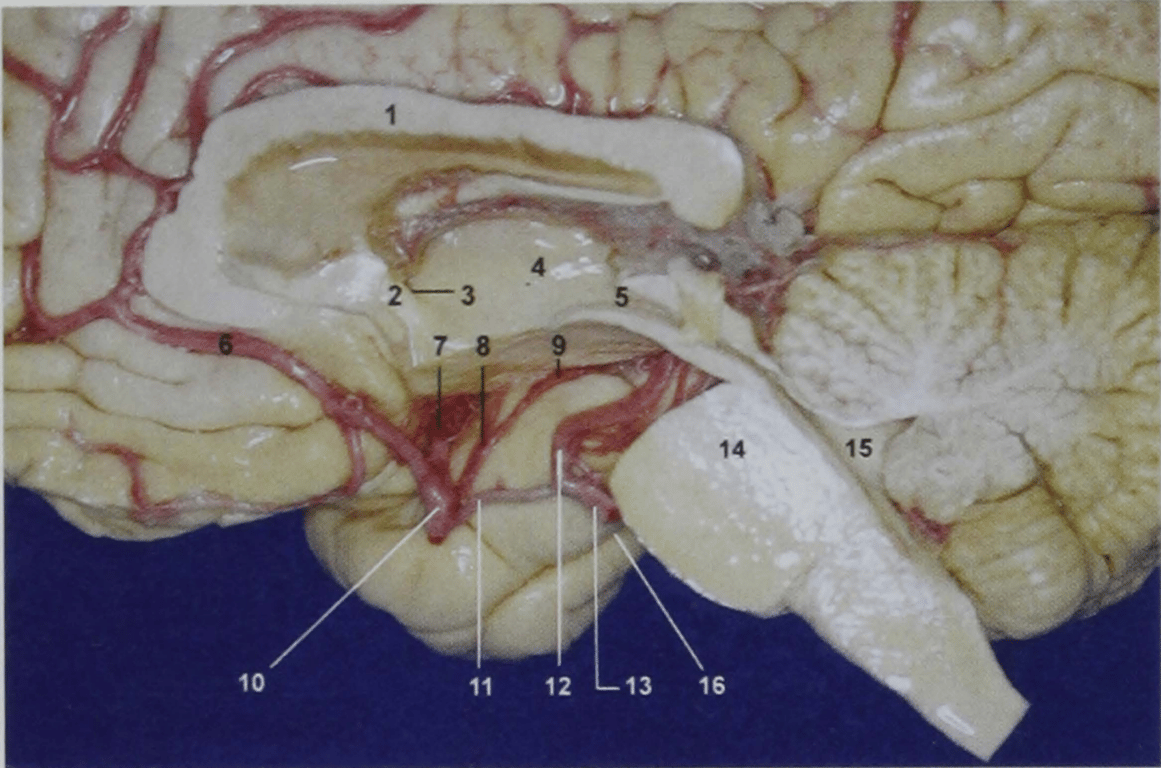
1, corpus callosum
2, fornix column and anterior commissure
3, foramen of munro
4, thalamus
5, aqueduct
6, ACA
7, MCA
8, Anterior choroidal artery (cisternal segment)
9, distal portion of the cisternal segment of the anterior choroidal artery (on the upper portion of the posteromedial surface of the uncus) entering the temporal horn
10, ICA
11, PCOM
12, P2A
13, P1
14, Tegmentum/pons
15, 4th ventricle
16, Rhinal sulcus
2, fornix column and anterior commissure
3, foramen of munro
4, thalamus
5, aqueduct
6, ACA
7, MCA
8, Anterior choroidal artery (cisternal segment)
9, distal portion of the cisternal segment of the anterior choroidal artery (on the upper portion of the posteromedial surface of the uncus) entering the temporal horn
10, ICA
11, PCOM
12, P2A
13, P1
14, Tegmentum/pons
15, 4th ventricle
16, Rhinal sulcus
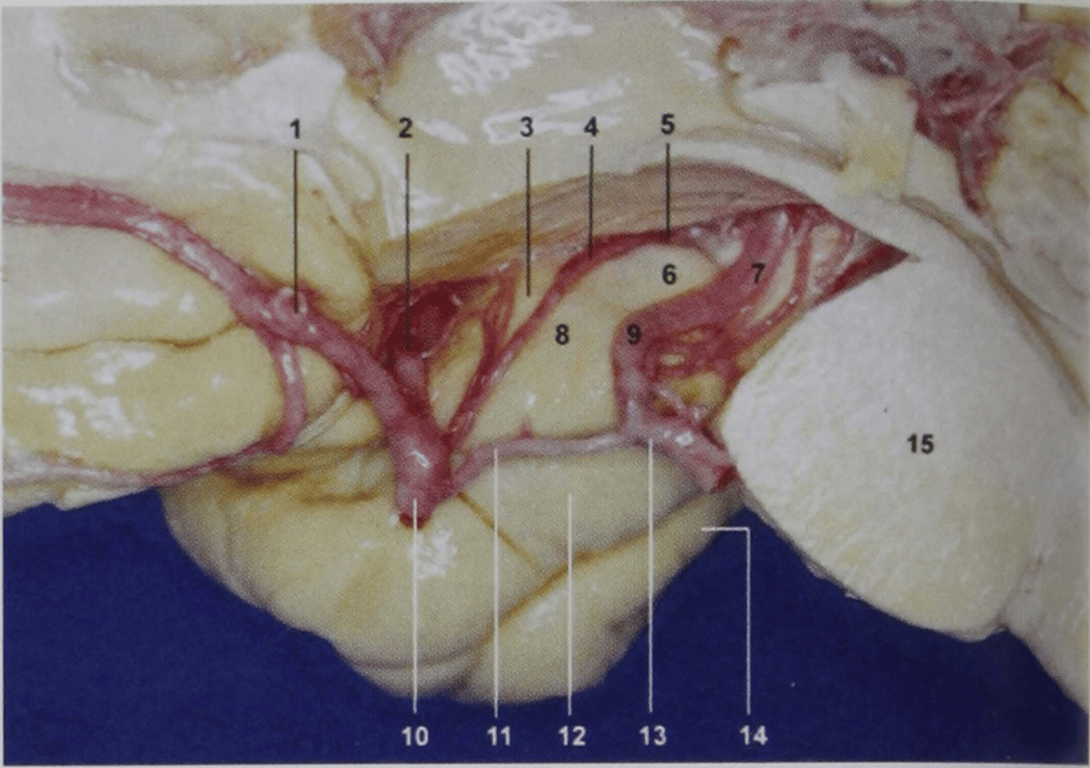
1, Acom
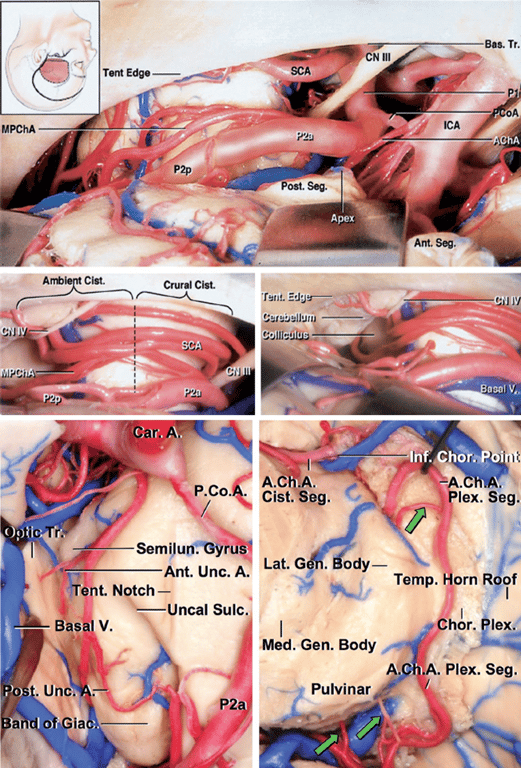
2, MCA
3, semilunar gyrus
4, Cisternal segment of anterior choroidal artery
5, inferior choroidal point
6, Posterior medial surface of uncus
7, P2P
8, ambient gyrus
9, P2A
10, ICA
11, PCOM
12, parahippocampal gyrus
13, P1
14, Fusiform gyrus (Collateral gyrus)
15, pons
2, MCA
3, semilunar gyrus
4, Cisternal segment of anterior choroidal artery
5, inferior choroidal point
6, Posterior medial surface of uncus
7, P2P
8, ambient gyrus
9, P2A
10, ICA
11, PCOM
12, parahippocampal gyrus
13, P1
14, Fusiform gyrus (Collateral gyrus)
15, pons
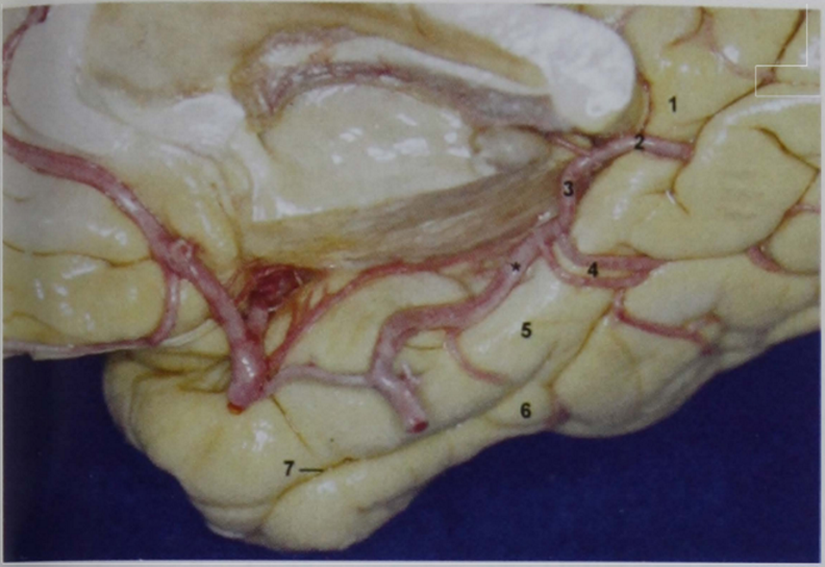
1, Isthmus of cingulate gyrus
2, P3
3, P3
4, Inferior temporal artery
5, Parahippocampal gyrus
6, collateral gyrus (fusiform gyrus)
7, Rhinal sulcus
*, P2P
2, P3
3, P3
4, Inferior temporal artery
5, Parahippocampal gyrus
6, collateral gyrus (fusiform gyrus)
7, Rhinal sulcus
*, P2P
Choroidal C7
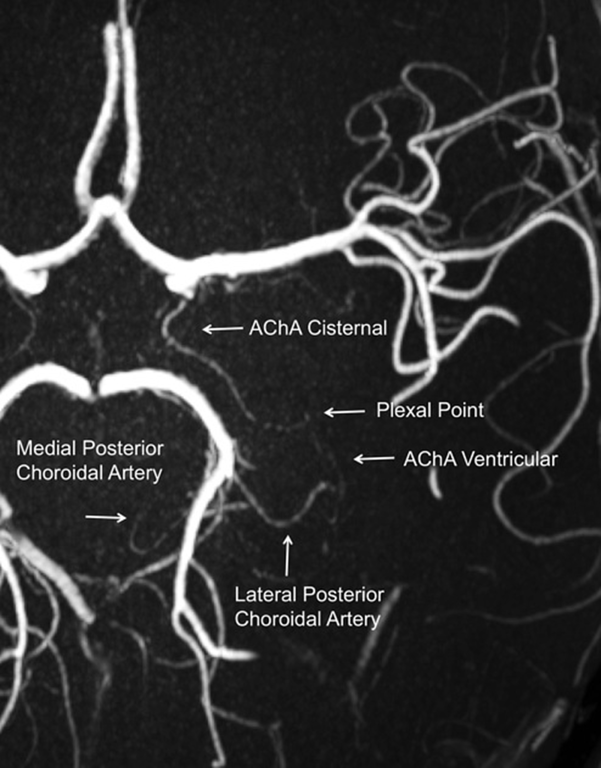
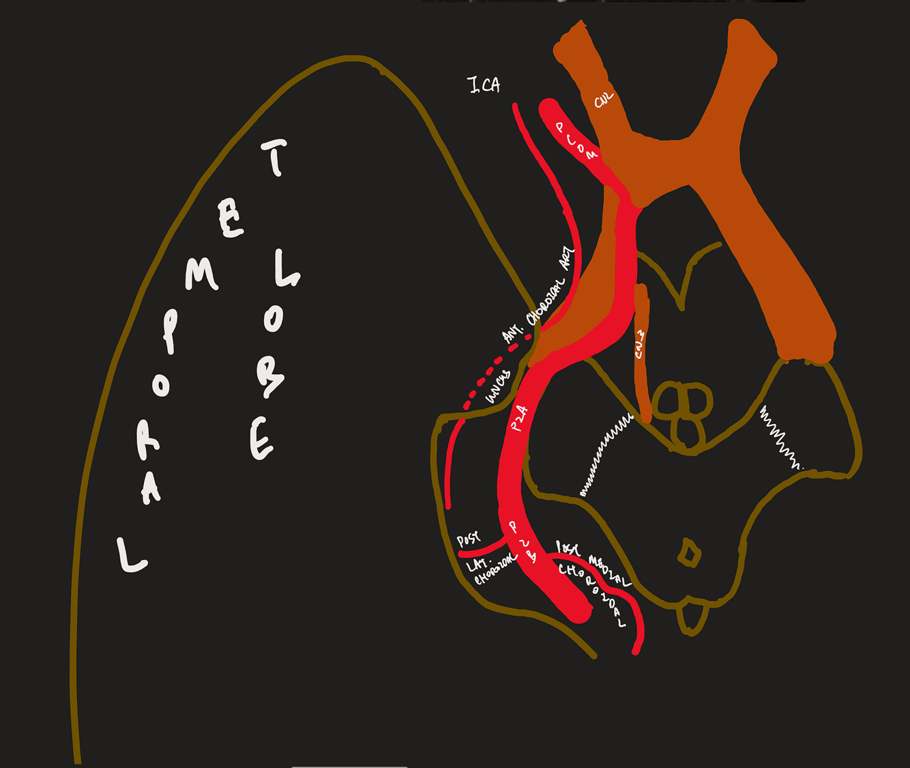
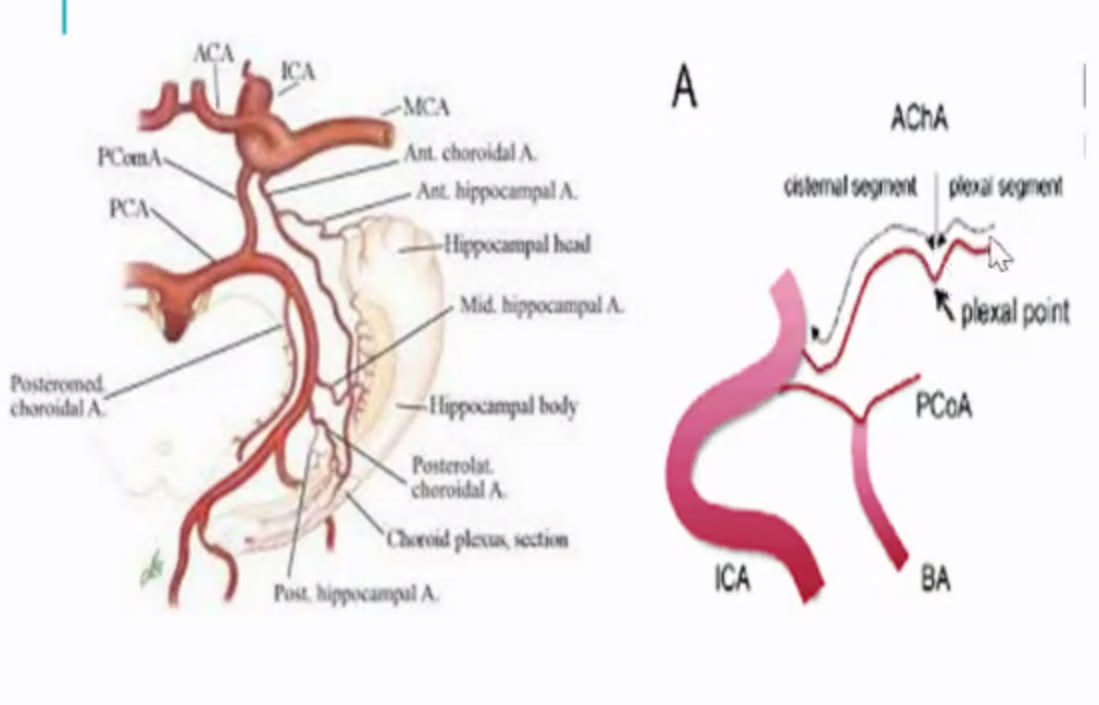
Anterior choroidal artery (ACh)
- Origin
- (1–3 mm distant to the PComA origin) usually arises from the posterior aspect of the ICA
- Course:
- Lateral to optic tract, curves medially to be inferomedial to optic tract --> curve laterally to run along the lateral aspect of the optic tract --> circumvents the cerebral peduncles to reach the lateral geniculate body --> traverses in the posterolateral direction above the uncus to enter the choroidal fissure, at the plexal point.
- Plexal point is always constant
- Two segments
- Cisternal segment:
- Extends from its origin until the choroidal fissure; measures ~2.5 cm
- Plexal/Intraventricular segment (3-10 perforators)
- Plexal point: where anterior choroidal artery enter temporal horn
- Supplies
- Visual system: Inferior optic chiasm, Posterior portion of optic tract, Optic radiation, Lateral geniculate body
- Temporal lobe: Uncus, Parahippocampal gyrus, Amygdala, Choroid plexus, Temporal horn, Atrium
- Basal ganglia: Globus pallidus medial, Tail of caudate, Internal capsule (genu)
- Diencephalon: Subthalamus, Thalamus (Lateral ventrolateral nucleus, Lateral ventroanterior nucleus)
- Midbrain: Middle 1/3 of cerebral peduncle, Upper red nucleus, Substantia nigra
- Very rare to have perforating branches outside of origin of anterior choroidal artery
- Anastomoses with lateral posterior choroidal artery
- Anterior choroidal artery-Clinical
- Use to be ligated to tx Parkinson's in the past
- Aneurysm: located superior/superiorlaterally to origin of anterior choroidal artery
- Stroke → Anterior choroidal artery syndrome: (3H)
- Hemisensory loss
- Hemiplegia
- Homonymous hemianopia
Difference between PCOM vs Anterior choroidal artery
Features | Anterior choroidal | PComA |
Origin | More distal | More proximal |
Size | Smaller | Larger |
Direction of travel | Has a superior hump (plexal point) where it passes through the inferior choroidal point to enter the temporal horn. | Goes up and down the straight back up and usually bifurcates |
Relation between each | More lateral | More medial |
Terminating
- Bifurcates in the area below the anterior perforated substance at the medial end of the sylvian fissure
 Made with Bullet
Made with Bullet