Definition
- A complex malformation that is invariably associated with myelo-meningocele and with multiple other brain anomalies.
Pathophysiology
- Mcline and Knepper Unified Theory/Hydrodynamic Oligo-CSF
- Neurulation is the primary defect.
- Gaining support from in utero fetal myelomeningocoele repair
- Observed resolution of Chiari Il after closure of the caudal defect
--- config: layout: dagre --- flowchart TD A["Lack of expression of<br>surface molecules<br>required for neural<br>tube closure"] --> B["Incomplete occlusion<br>of neural tube → CSF<br>leakage"] B --> C["ICP hypotension<br>in the ventricular<br>system"] %% Nodes branching from C: C --- D2["In the 3rd ventricle"] C --- n2["In the lateral ventricle"] C --- n6["In the posterior fossa"] %% Branches from D2: D2 --> n3["3rd ventricle is not<br>inflated adequately"] n3 --> n4["Extended<br>thalamic contact"] n4 --> n5["Enlargement of massa<br>intermedia"] %% Branches from n2: n2 --> D1["Germinal matrix<br>disruption at lateral<br>ventricle"] D1 --> n1["Malformation of cortical<br>development"] %% Branches from n6: n6 --> D3["Rhombencephalic<br>vesicle fails to<br>expand"] D3 --> E["No induction of<br>posterior fossa<br>perineural mesenchyma"] E --> F["Smaller posterior<br>fossa"] F --> G["Unable to accommodate<br>developing<br>rhombencephalon"] G --> H["Displacement of<br>cerebellum and<br>brainstem"] %% Branches from H: H --- I["Upwards through<br>tentorium"] H --- J["Downwards through<br>foramen magnum"] %% Branches from I and J: I --> n7["Large tentorial<br>incisura /<br>towering cerebellum"] J --> n8["Tonsillar and<br>medullary<br>displacement"] %% Node styles: style D2 fill:#FFD600 style n2 fill:#FF6D00 style n6 fill:#00C853 style n1 shape:rect style n3 shape:rect style n4 shape:rect style n5 shape:rect style n7 shape:rect style n8 shape:rect
- Traction theory: primary defect is tethering of the spinal cord which leads to abnormal traction and pulling of the posterior fossa contents into the cervical canal.
- Less supported
Main features

- Caudally dislocated
- Cervicomedullary junction
- Pons
- 4th ventricle: Tube like elongated (4)
- Medulla (9)
- Cerebellar tonsils located at or below the foramen magnum (3)
- Replacement of normal cervicomedullary junction flexure with a “kink-like deformity.” (9)
- Other possible associated findings:
- Colpocephaly (1)
- congenital brain abnormality in which the occipital horns are larger than normal because white matter in the posterior cerebrum has failed to develop or thicken.
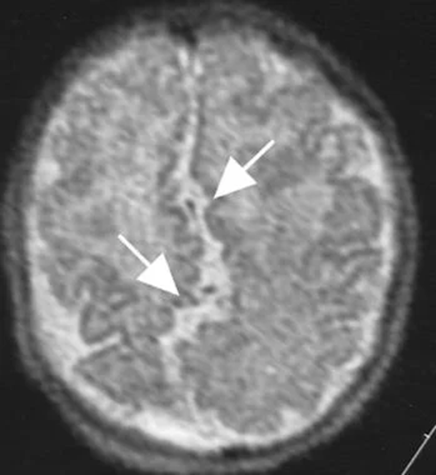
- Beaking of tectum (2): small arrow
- Absence of the septum pellucidum with enlarged interthalamic adhesion (large arrow):
- Due to necrosis with resorption secondary to hydrocephalus,
- not a congenital absence
- Poorly myelinated cerebellar folia
- Hydrocephalus: present in most
- Heterotopias
- Hypoplasia of falx
- Microgyria
- Degeneration of lower cranial nerve nuclei
- Cerebellar hemispheres wrapping around the brainstem anteriorly (6)
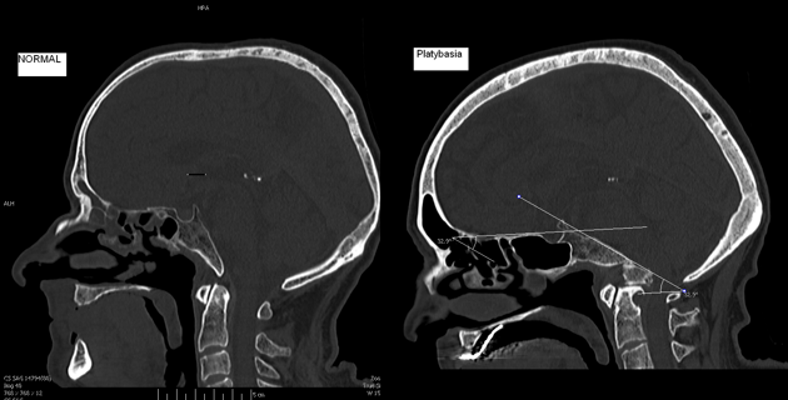
- Concave clivus (7)
- Bony abnormalities:
- Assimilation of atlas
- Platybasia
- Basilar impression
- Klippel-Feil deformity
- Syringomyelia
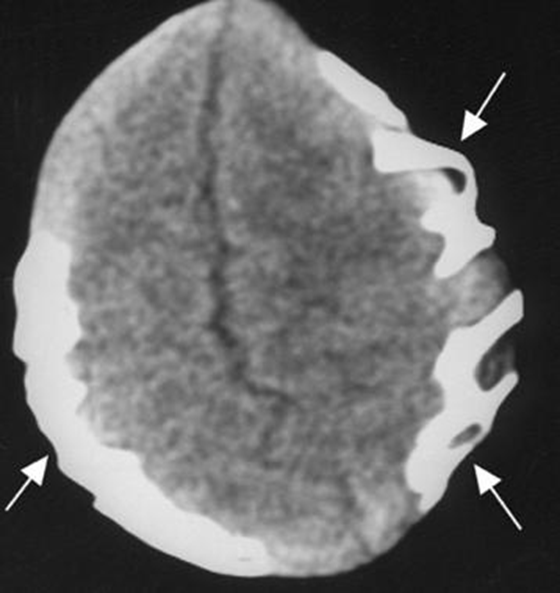
- Craniolacunia of the skull
- Low lying torcula herophil (5)

Presentation (complex)
Due to
- Brain stem and lower cranial nerve dysfunction
Late problems
- Hydrocephalus
- Syringomyelia/syringobulbia
- Tethered cord syndrome
- Symptomatic Chiari II
- Rule out shunt malfunction when chiari II patient deteriorates
Age
Neonates
- Rapid deterioration
- swallowing difficulties (neurogenic dysphagia)
- 69%
- Manifests as
- Poor feeding
- Cyanosis during feeding
- Nasal regurgitation
- Prolonged feeding time
- Pooling of oral secretions
- Gag reflex often decreased.
- Apneic spells
- 58%
- due to impaired ventilatory drive
- Stridor
- 56%
- Worse on inspiration (abductor and occasionally adductor vocal cord paralysis seen on laryngoscopy)
- Due to 10th nerve paresis;
- usually transient, but may progress to respiratory arrest
- Aspiration
- 40%
- Downbeat nystagmus
- weak or absent cry
Childhood
- Progressive spastic weakness
- Arm weakness (27%) that may progress to quadriparesis
- Facial weakness
- Opisthotonous
- 18%
- Gradual appendicular ataxia.
Teenagers
- Insidious onset gait difficulty and truncal ataxia
Adults
- Symptoms tend to stabilize
- Rare presentation
Diagnostic investigation
Skull films
- Cephalofacial disproportion from congenital HCP
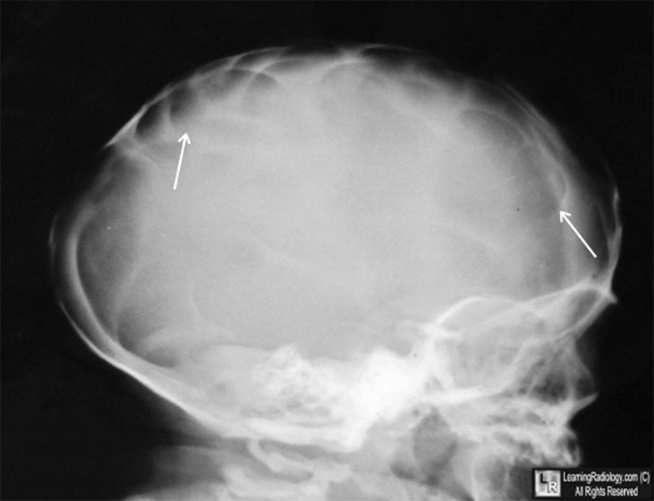
- Lacunar skull (aka Lückenschädel)
- 85%
- Round defects in the skull with sharp borders, separated by irregularly branching bands of bone; Not due to increased ICP
- Low lying internal occipital protuberance (foreshortened posterior fossa).
- Enlarged foramen magnum in 70%
- Elongation of upper cervical lamina.
CT and/or MRI findings
- Cranial and cervical MRI is the diagnostic test of choice
Features classified by location
Supratentorial
- Obstructive hydrocephalus
- Corpus callosal agenesis and absent septum pellucidum
- Stenogyria/polymicrogyria
- enlarged massa intermedia (interthalamic adhesion)
- Fenestration of falx cerebri with interdigitation of gyri
Posterior fossa
- Small posterior fossa with low-lying tentorium and torcula
- Herniation of the cerebellar tonsils and vermis through widened foramen
- Brainstem appears pulled down with elongated 4th ventricle
- Tectal beaking: inferior colliculus elongated posteriorly causing angulation and stenosis of aqueduct resulting in hydrocephalus
- Trapped fourth ventricle
- Cervicomedullary kinking (as dentate ligament stops cord descending further)
- “Z” bend deformity of medulla*
- Scalloping of petrous temporal bone
Spinal
- Myelomeningocele
- Syringomyelia in the area of the cervicomedullary junction
- Reported incidence in pre-MRI era: 48–88%
- Klippel-Feil syndrome, scoliosis
Treatment
General
- Insert CSF shunt
- for hydrocephalus (or check function of existing shunt)
- If neurogenic dysphagia, stridor, or apneic spells occur, expeditious posterior fossa decompression is recommended (required in 18.7% of MM patients);
- Before recommending decompression, always make sure the patient has a functioning shunt!
- Tracheostomy
- (usually temporary)
- is recommended if stridor and abductor laryngeal palsy are present pre-op.
- Close post-op respiratory monitoring is needed for obstruction and reduced ventilatory drive
- Mechanical ventilation is indicated for hypoxia or hypercarbia.
Foramen magnum decompression
- It has been argued that part of the explanation for the poor operative results in infants is that many of the neurological findings may be due in part to intrinsic (un-correctable) abnormalities which surgical decompression cannot improve.
- Expeditious brainstem decompression should be carried out when any of the following critical warning signs develop:
- Neurogenic dysphagia
- Stridor
- Apneic spells
Prevention
- Prenatal myelomeningiocele repair
Outcome
- 68% had complete or near-complete resolution of symptoms,
- 12% had mild to moderate residual deficits,
- 20% had no improvement
- Neonates fared worse than older children
- Mortality
- Respiratory arrest is the most common cause of mortality (8 of 17 patients who died)
- Meningitis/ventriculitis (6 patients)
- Aspiration (2 patients)
- Biliary atresia (1 patient)
- In follow-up ranging 7 mos-6 yrs,
- 37.8% mortality in operated patients.
- Prognostic factor
- Pre-op status
- Bilateral vocal cord paralysis
- Rapidity of neurologic deterioration
- 71% in infants with more acute deterioration (2 weeks of presentation)
- Cardiopulmonary arrest,
- Vocal cord paralysis
- Arm weakness
- 23% in patients with a more gradual deterioration.
 Made with Bullet
Made with Bullet