General
- An extremely rare condition
- This malformation is rarely compatible with life.
Main feature
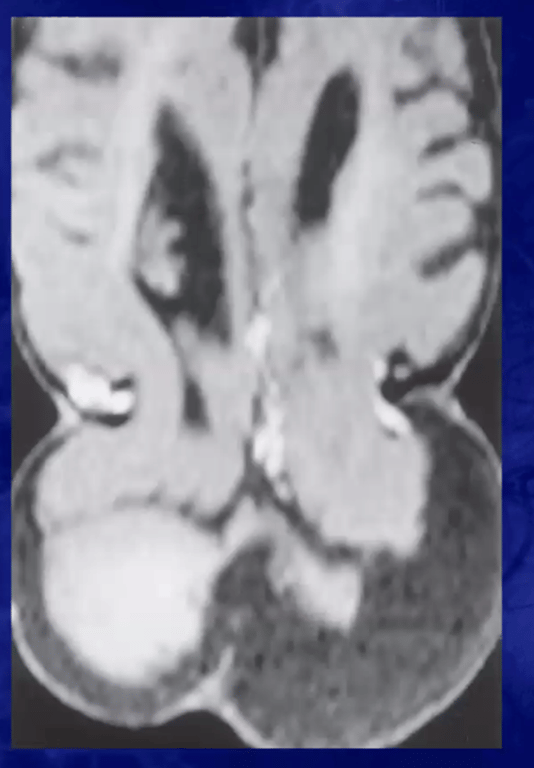
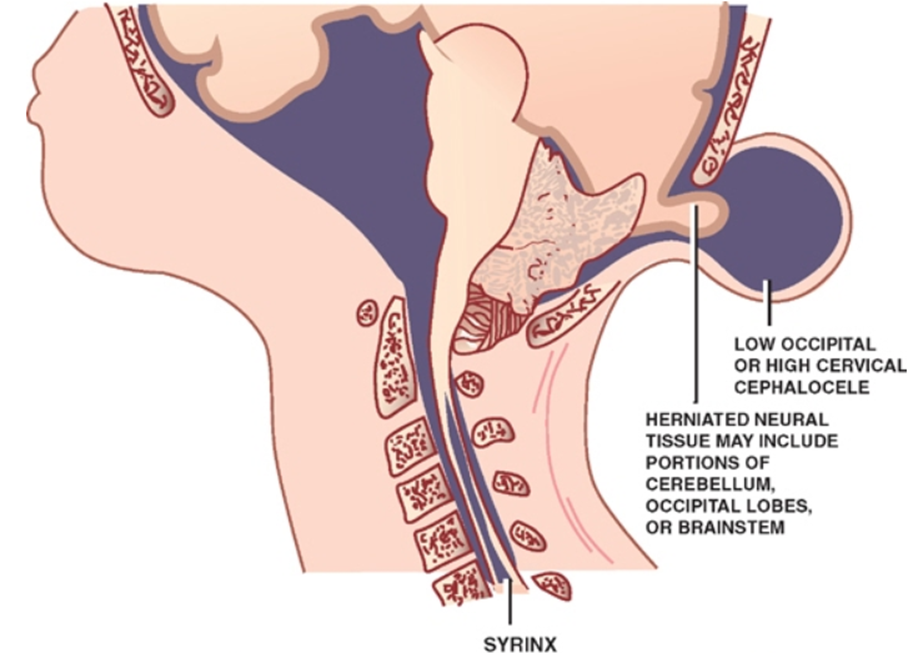
- Herniation of posterior fossa contents (cerebellum, pons and medulla) through a spina bifida defect at the C1–C2 level (encephalocele).
- Herniated contents is grossly abnormal and often non functioning
- In the most severe presentations, the herniated tissue within the encephalocele can include the brainstem, occipital lobes, parietal lobes, dural venous sinuses, and subarachnoid spaces.
Associated features
Hindbrain Displacement:
- The displacement of the cerebellum, brainstem, and fourth ventricle extends into the cervical canal, frequently reaching the C3–C5 level or even more. The herniating tissue realizes a posterior cranial fossa (PCF) encephalocele through a bony defect.
Bony anomalies:
- C-III is typically characterized by an undersized PCF
- An enlarged foramen magnum.
- Scalloping of the clivus.
- Hypoplasia of the parietal bones and possible posterior cervical agenesis (missing posterior elements from C1 to C5).
- Lückenshädel (thinning or erosion of the skull).
Intracranial anomalies
- Medullary kinking.
- Tectal beaking.
- Callosum dysgenesis.
- Colpocephaly.
- Hydrocephalus, which is present in up to 88% of cases.
Associated Spinal Anomalies:
- Syringomyelia is common, occurring in up to 70% of cases.
- Associated anomalies may include Dandy-Walker malformation, Klippel-Feil syndrome, and split cord malformation.
Pathogenesis
- The most advocated theory is that C-III results from a chronic escape of cerebrospinal fluid (CSF) at the occipito-cervical neural tube defect level. This leakage causes the underdevelopment of the cerebral ventricle and posterior cranial fossa.
- Alternatively, the malformation may stem from a primary neuroectodermal defect resulting in abnormal neurulation and consequent PCF hypoplasia, or a primary mesodermal defect leading to bone deficiency.
Prognosis and Outcome
- Mortality:
- There is a high risk of spontaneous and surgical mortality (overall rate of 29%).
- Negative Prognostic Factors:
- These include stridor at birth, poor neurological status prior to surgery, large encephalocele, and hydrocephalus.
- The amount of herniating brainstem is crucial; a better outcome is registered if the ectopia is less than 5 cm.
- Long-term Sequelae:
- Surviving children almost invariably experience developmental delay, motor deficits, lower cranial nerve deficits, and epilepsy.
- These neurological issues are generally attributed to primary brainstem dysfunction or secondary damage from distortion and traction of the brainstem caused by the malformation.
 Made with Bullet
Made with Bullet