General
- Aka: cephalocele
Definition
- Encephaloceles
- Skull-base or skull defect causing herniation of intracranial contents.
- Meningoencephalocele
- If the herniated contents contain both meninges and brain tissue
- Meningiocele
- If the herniated contents contain meninges only
- Cranium bifidum
- A defect in the fusion of the cranial bone
- Occurs in the midline
- Most common in the occipital region
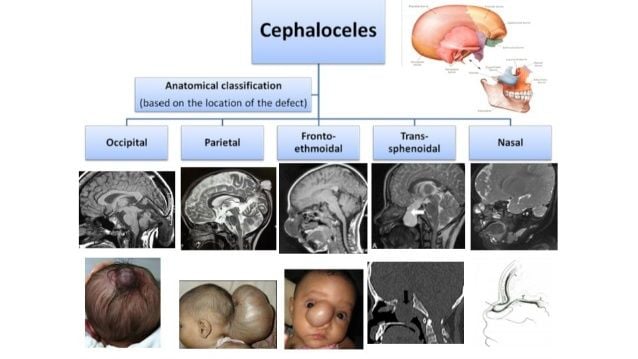
Classification
By contents
- Meningocele
- Contains CSF and lined by meninges
- Gliocele
- Contains CSF and lined by glial tissue
- Encephalocele (meningoencephalocele)
- Contains CSF and brain
- Meningoencephalocystocele
- Contains CSF, brain and ventricles
- Atretic cephalocele
- Small nodule of fibrous fatty tissue
Suwanwela Classification (by location)
--- config: layout: dagre --- flowchart TD A["Encephaloceles<br>"] --> A1["Occipital<br>"] & A2["Sincipital<br>"] & A3["Convexity<br>"] & A4["Basal<br>"] A2 --> B1["Frontoethmoidal<br>encephaloceles"] & B2["Interfrontal<br>encephaloceles"] & B3["Associated with<br>craniofacial clefts"] B1 --> C1["Nasofrontal<br>"] & C2["Nasoethmoidal<br>"] & C3["Naso-orbital<br>"]
Types of encephalocele
Numbers
- One case was seen for every five cases of spinal myelomeningoceles
- Incidence is 1 in 10,000—1 in 1000
- Commonest in Europe and North America
Pathogenesis
- Arrested closure of normal confining tissue allows herniation through persistent defect
- Early outgrowth of neural tissue prevents normal closure of cranial coverings
- Depending on their location.
- Skull-base cephaloceles
- Due to
- Failure of induction of bone due to faulty neural tube closure
- Disunion of basilar ossification centres.
- Leading to defects of endochondral bone
- Calvarial cephaloceles
- Due to
- Defect of bone induction
- Nonseparation of neural and surface ectoderm leading to defective formation of the occipital bone.
- Mass effect and pressure erosion of bone by an expanding intracranial lesion,
- Failure of neural tube closure
- Similar to cranial dermal sinus
- Leading to defects of membranous bone
Clinical features
- A nasal polypoid mass in a newborn should be considered an encephalocele until proven otherwise
Treatment
- Occipital encephalocele
- Surgical excision of the sac and its contents with water-tight dural closure.
- Normally opening is very small just ligate the encephalocele and cut excess skin and Dura and brain and close.
- Caution: vascular structures are often included in the sac.
- Hydrocephalus is often present and may need to be treated separately.
- Basal encephalocele
- Caution: a transnasal approach to a basal encephalocele (even for biopsy alone) may be fraught with intracranial hemorrhage, meningitis, or persistent CSF leak.
- Usually a combined intracranial approach (with amputation of the extracranial mass) and transnasal approach is used.
Outcome
- Occipital encephalocele
- The prognosis is better in occipital meningocele than in encephalocele.
- Poor prognosis
- Significant amount cerebral tissue is present in the sac,
- If the ventricles extend into the sac, or
- If there is hydrocephalus.
- <5% of infants with encephalocele develop normally.
Differential diagnosis
- How can one differentiate a nasal polyp from a sincipital encephalocele?
ㅤ | Encephalocele | Polyp |
Pulsate | Yes | No |
Location (from nasal septum) | Medially | Laterally |
Nasal bridge | Widens | Does not widen |
 Made with Bullet
Made with Bullet