General
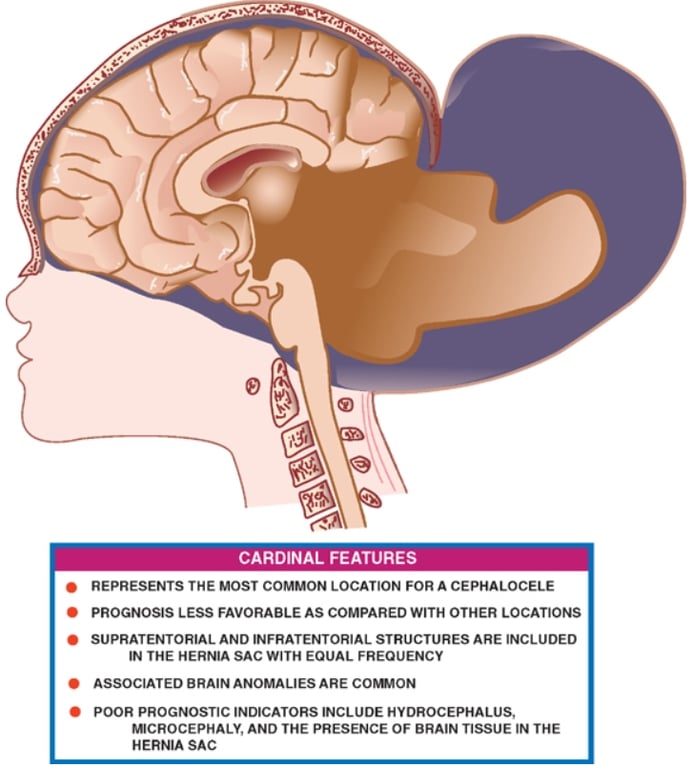
- Most common location
- Often involves vascular structures
- Often large
- Usually covered with normal skin and hair, with herniation of the infra and/or supratentorial structures through a narrow pedicle.
- Less favourable prognosis vs other locations.
Contents
- Supratentorial and infratentorial structures with equal frequency.
- Dural venous sinus can be included in the herniated sac
- Herniated brain tissue may be normal, dysplastic, or may show new/old ischemic or hemorrhagic changes
- Because of strangulation of the blood vessels at the neck of the sac.
- The tentorium is frequently reduced into crescentic folds and is inserted inferior to the petrous ridge, leading to a narrow, funnel-shaped lower posterior fossa.
- The falx is usually thin, hypoplastic, and may either attach to the superior margin of the defect or herniate into the encephalocele.
- Because of traction, the cerebral parenchyma is pulled posteriorly, and nonherniated brain may assume abnormal positions in the skull.
- The anterior commissure, septum pellucidum, and fornices are absent in 80% of cases.
Commonly associated brain anomalies
- Anomalies of neuronal migration,
- Chiari malformations
- Type III Chiari malformation
- Includes an occipital or cervicooccipital encephalocele with herniation of the medulla, 4th ventricle and cerebellum, and sometimes the occipital lobes (rare)
- Dandy Walker malformation
- Hydrocephalus may affect the entire ventricular system or it may be limited to the extracranial portion of the ventricles.
- Cerebellar cortical dysplasia,
- Heterotopias
- Partial/complete absence of corpus callosum may be seen.
 Made with Bullet
Made with Bullet