General
- Definition: Absent cerebral hemisphere
Pathology
- A post-neurulation defect.
- vs anencephaly: where brain does not develop
- Total or near-total absence of the cerebrum (small bands of cerebrum may be consistent with the diagnosis), with intact cranial vault and meninges, the intracranial cavity being filled with CSF.
- Presence of progressive macrocrania, but head size may be normal (especially at birth),
- occasionally, microcephaly may occur.
- Facial dysmorphism is rare.
Etiology
- bilateral ICA infarcts → Absence of brain tissue supplied by the anterior and middle cerebral arteries with preservation in the distribution of the PCA
- Most common
- Infection (congenital or neonatal herpes, toxoplasmosis, equine virus).
Clinical features
- Less affected infants may appear normal at birth, but are often hyperirritable and retain primitive reflexes (Moro, grasp, and stepping reflex) beyond 6 mo.
- They rarely progress beyond spontaneous vowel production and social smiling.
- Seizures are common.
Differentiation from severe (“maximal”) hydrocephalus
- Progressive enlargement of CSF spaces may occur, which can mimic severe (“maximal”) hydrocephalus (HCP).
- It is critical to differentiate the two, since true HCP may be treated by shunting, which may produce some re-expansion of the cortical mantle.
- EEG
- The best ways to differentiate the two
- shows no cortical activity in hydranencephaly (maximal HCP typically produces an abnormal EEG, but background activity will be present throughout the brain)
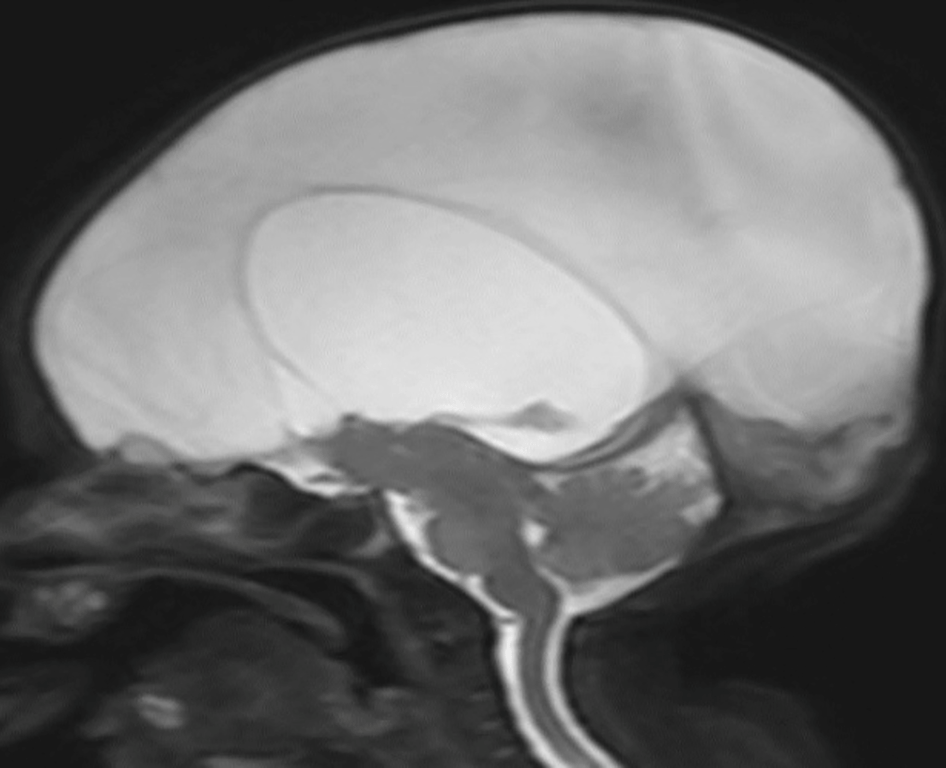
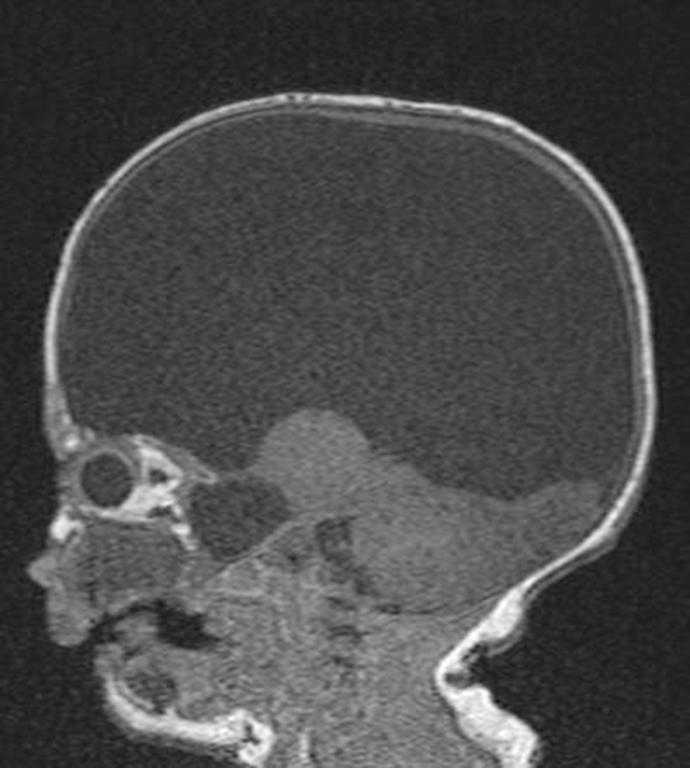
- CT, MRI, or U/S:
- majority of intracranial space is occupied by CSF.
- Usually do not see frontal lobes or frontal horns of lateral ventricles (there may be remnants of temporal, occipital or subfrontal cortex).
- A structure consisting of brainstem nodule (rounded thalamic masses, hypothalamus) and medial occipital lobes sitting on the tentorium occupies a midline position surrounded by CSF.
- Posterior fossa structures are grossly intact.
- The falx is usually intact (unlike alobar holoprosencephaly) and is not thickened, but it may be displaced laterally.
- In HCP, some cortical mantle is usually identifiable
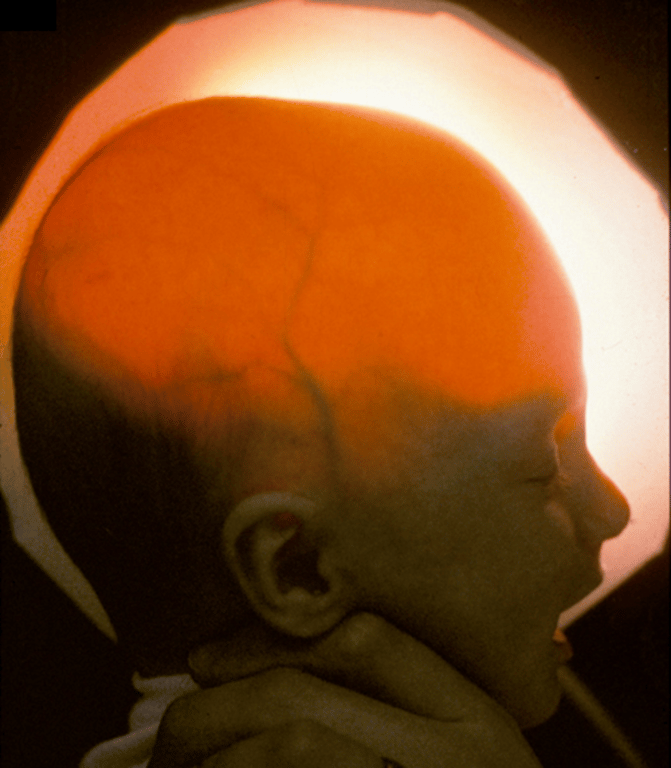
- Transillumination of the skull:
- in a darkened room, a bright light is placed against the surface of the skull.
- To transilluminate, the patient must be< 9 mos old and the cortical mantle under the light source must be <1cm thick, but it can also occur if fluid displaces the cortex inward (e.g. subdural effusions).
- Too insensitive to be very helpful
- Angiography:
- in “classic” cases resulting from bilateral ICA occlusion, no flow through supraclinoid carotids and a normal posterior circulation is expected
Treatment
- Shunting may be performed to control head size, but unlike the case with maximal hydrocephalus, there is no restitution of the cerebral mantle.
 Made with Bullet
Made with Bullet