General
- Aka: enlarged cisterna magna
Definition
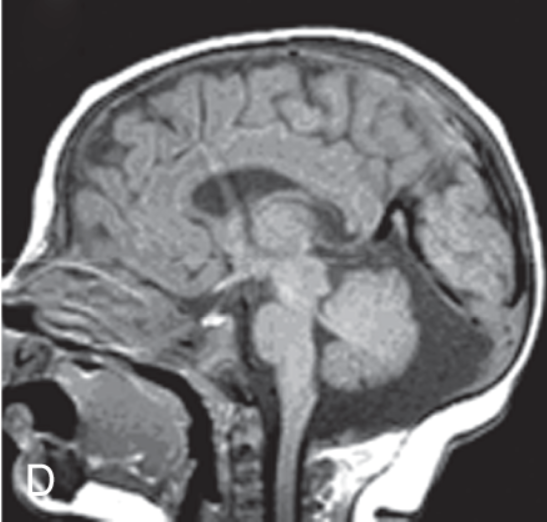
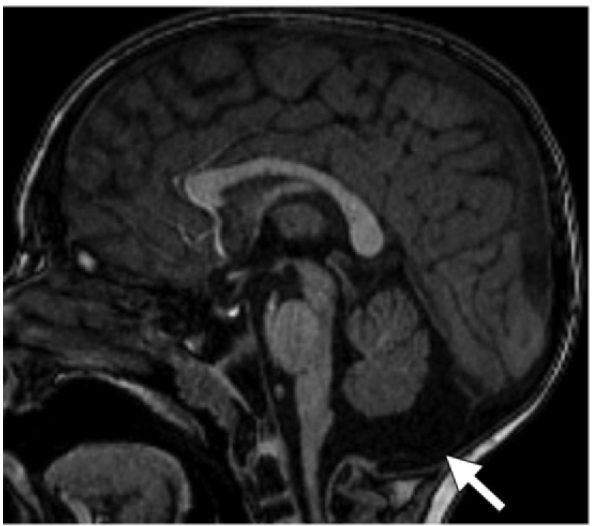
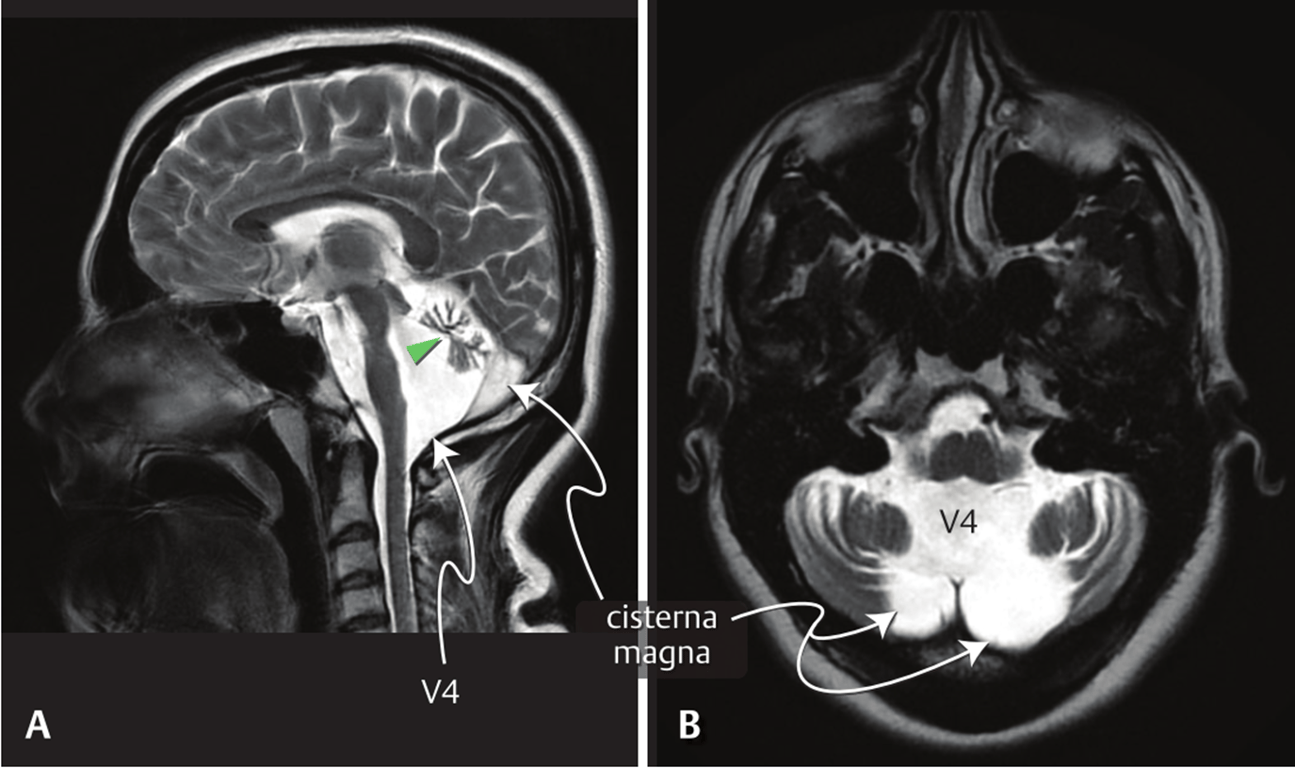
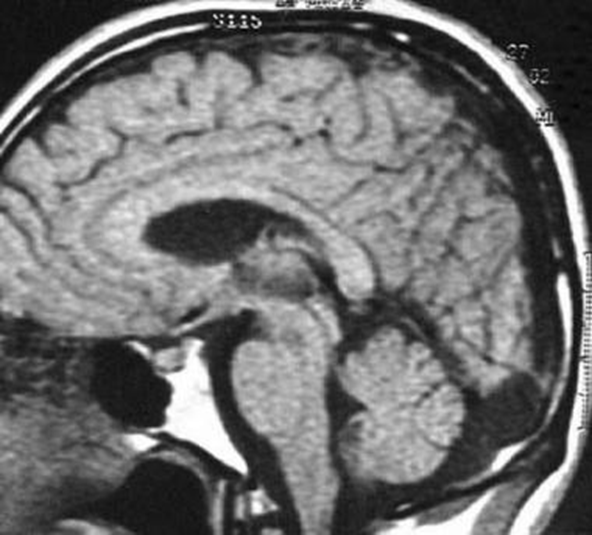
- an enlarged posterior fossa secondary to an enlarged cisterna magna (>10 mm on midsagittal images),
- A normal
- vermis
- 4th ventricle.
- in some patients, an enlarged posterior fossa
Pathology
flowchart LR C[Non-perforation of<br>foramen of Magendie] C --> D[4th ventricle enlargement] D --> E[Foramina of Luschka<br>eventually opens] E --> F[CSF flow from 4th<br>into cisterns] F --> G[Focal enlargement of the<br>subarachnoid space in the<br>inferior & posterior portions<br>of the posterior fossa] G --> H[Mega cisterna magna freely<br>communicates with 4th and<br>cervical subarachnoid space]
Mega cisterna magna freely communicates with the fourth ventricle and the cervical subarachnoid space (can be seen on MRI-CISS studies)
Presentation
- Incidental finding and represents a normal variant
Evaluation
- Imaging
- normal
- vermis
- No hydrocephalus
- Abnormal
- enlarged posterior fossa secondary to an enlarged cisterna magna.
- Normal vermis and fourth ventricle and no mass effect on the cerebellum
Clinical features
- Incidental (asymptomatic)
- Ventriculomegaly occurs rarely (2.3%) before or after birth.
- Very similar to Blake's pouch cyst but mega cisterna magna has no HCP
Treatment
- There is no role for shunt surgery even if the cisterna magna is extremely large.
Outcomes
- no reported recurrence risk.
- 95 of children with isolated mega cisterna magna develop normally
 Made with Bullet
Made with Bullet