Normal 4th ventricular formation
- Blake’s pouch
- aka rudimental fourth ventricular tela choroidea
- is a normal transient structure during embryological development
- Regresses at 12 weeks of gestation
- Though a fenestration to form the foramen of Magendie (which forms in up to the fourth month of gestation).
- The foramina of Luschka open later than the foramen of Magendie during the embryologic development
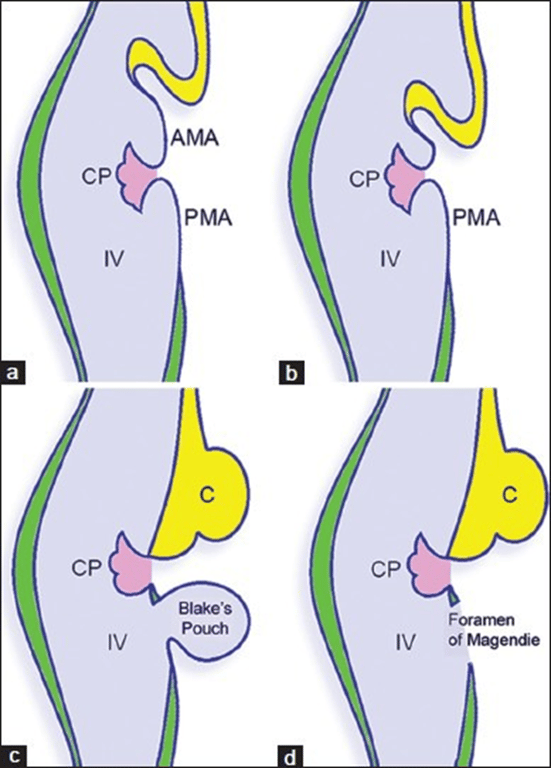
- Embryonic sequence of events in the development of the roof of the fourth ventricle.
- The plica choroidea (choroid plexus) divides the roof of the fourth ventricle into an anterior membranous area and a posterior membranous area (a).
- The cerebellar vermis originates from the anterior membranous area (b), which eventually disappears.
- Blake's pouch appears as a protrusion of the posterior membranous area of the fourth ventricular roof (c), which later communicates with the subarachnoid space forming the foramen of Magendie (d).
Definition
- Ballooning of the inferior medullary velum due to an imperforated foramen of Lushka and magendie.
Mechanism
- Absence in fenestration of the Blake's pouch
Numbers
- Rare
Clinical presentation
- Asymptomatic
- If there is adequate flow through foramen of Lushka
- hydrocephalus (usually headache, vomiting, blurred or double vision)
- More likely to be present in blake pouch cyst rather than mega cisterna magna.
- MRI cannot differentiate Mega cisterna magna from persistent blake pouch cyst
- Macrocephaly
Imaging
- MRI
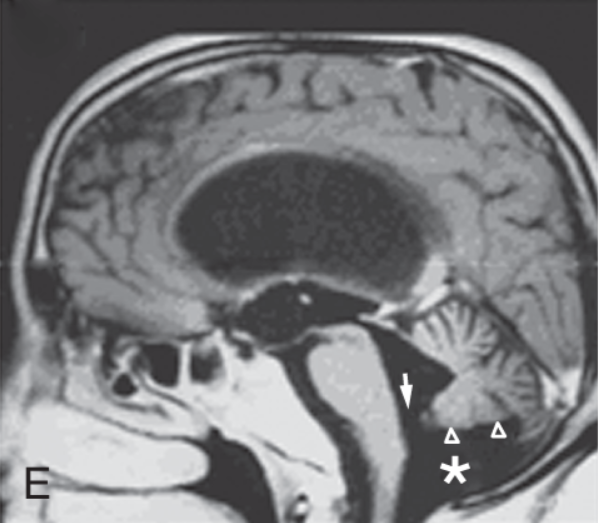
- Infravermian cyst that communicates with fourth ventricle (or a 4th ventricular diverticulum)
- choroid plexus can extend from fourth ventricle → superior portion of cyst,
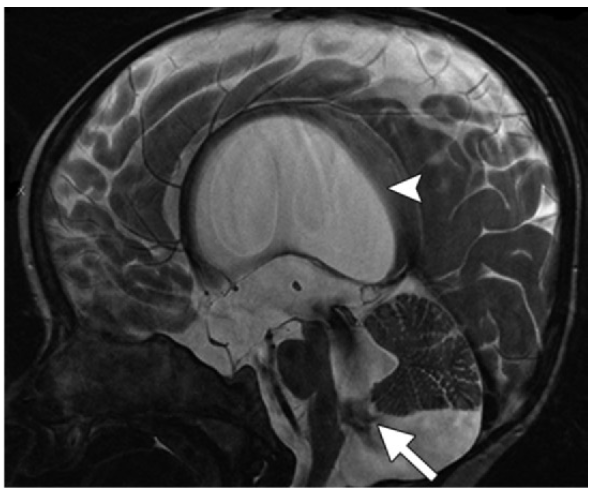
- cyst is smooth with thin walls that can be visualised on thin sagittal T2 images
- it can impress on medial side of cerebellar tonsils due to size
- cyst does not communicate with the cisterna magna posteriorly
- upward displacement of the vermis
- Elevation of tentorium but with a normally positioned torcula
- Torcula is elevated in dandy walker
- CISS:
- can see a membrane at the craniocervical junction
- no vermian hypoplasia or rotation
- presence of a cyst in a retrocerebellar or infraretrocerebellar location, which is essentially a diverticulum of the consequently enlarged fourth ventricle
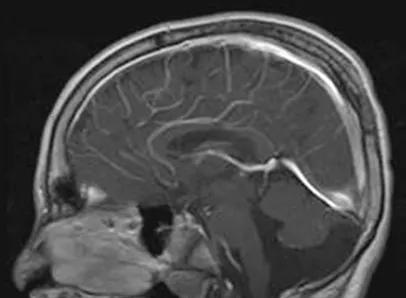
- choroid plexus in a Blake pouch cyst at times may be identified as being displaced into the cyst along its superior wall (under and posterior to the vermis),
- The displacement of the choroid plexus is best visualized as an enhancing structure on sagittal contrast material–enhanced T1-weighted images
- The consistent presence of hydrocephalus allows the differentiation of Blake pouch cyst from mega cisterna magna.
- Mild mass effect may result in indentation of the inferior vermis or of the caudal and medial aspects of the cerebellar hemispheres.
- The posterior fossa is typically normal in size.
- Supratentorial morphologic abnormalities other than hydrocephalus are usually absent.
- Hydrocephalus of all 4 ventricles
Treatment
- ETV
 Made with Bullet
Made with Bullet