Definition
- An AD mutation in the FGFR3 gene stuns long bone growth causing dwarfism (trident hands, short stature, large skull but small skull base)
Numbers
- Most common dwarfism
- Prevalence 1–20–30,000 live-born infants
Genetics
- Mutation in the fibroblast growth factor receptor FGFR 3 gene
- autosomal dominant (AD)
- a sporadic mutation initially in >80%, then AD
- risk increases with advanced paternal age
- caused by G380 mutation of FGFR3 (fibroblast growth factor receptor 3, on chromosome 4p16.3)
- FGFR3 is an important negative regulator of linear bone growth by decreasing chondrocyte proliferation and differentiation in the growth plate
- gain of function mutation that increases inhibition of chondrocyte proliferation in the proliferative zone of the physis
- results in defect in endochondral bone formation
- a quantitative cartilage defect
- Associated conditions
Clinical features
- Symptoms
- normal intelligence
- Delayed motor milestones
- Spinal stenosis
- pseudoclaudication and standing discomfort
- numbness and paraesthesia
- subjective weakness
- System affected
- frontal bossing
- midfacial hypoplasia
- humerus shorter than forearm
- femur shorter than tibia
- normal trunk
- adult height ~ 50 inches
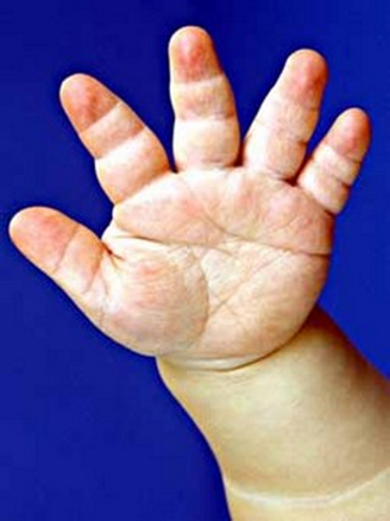
- trident hands (fingers same length with divergent ring and middle fingers)
- muscular hypotonia in infancy
- Genu varum
- Limited extension of the elbow
- Hyperextensibility of other joints
- Short fingers and hands (called the trident hand)
- Head size more than two standard deviations above the mean for age
- Very common hence achondroplasia patient have their own growth charts
- Head size is most often greatly increased and shows accelerated growth in early infancy;
- Own theory: ? Small skull base with compensatory enlargement of skull to accommodate normal brain size
- They have their own growth chart
- Enlarged brain with normal size or slightly enlarged ventricles
- is more common and presumably
- Due to
- chronic low-grade impairment in flow of venous blood from the brain and thus a low-grade increase in the pressure in the cranial sinuses.
- Clinical features seen in patients with increased intracranial venous pressure include
- dilated venous structures in the scalp and face,
- bulging anterior fontanelle, cranial bruit, and headache
- Enlarged head with enlarged ventricles
- MOST PT DO NOT HAVE HCP
- Due to
- Stenosis of foramen magnum and post fossa → communicating HCP (technically)
- This communicating hydrocephalus results in prominence of the subarachnoid spaces throughout the skull with mild ventricular enlargement
- stenosis of skull foramen → venous outflow obstruction → communicating HCP → Macrocephaly
- Most pt do not have HCP
- Shunting can lead to craniocerebral dysproportionism
- The most useful approach is to decompress the posterior fossa and foramen magnum allowing better drainage of the CSF and venous blood from the head.
Facial features
Extremities
Rhizomelic dwarfism

Cranial
Macrocephaly
Megalencephaly
Hydrocephalus
Managment
- Associated medical conditions
- weight control problems
- hearing loss
- tonsillar hypertrophy
- frequent otitis media
- Infertility
- decreased reproductive efficiency in patients with achondroplasia,
- 50% chance of the product of a pregnancy occurring as a result of mating between two individuals with achondroplasia
- The possibility of the fetus being homozygous for the mutation is about 25% but such an unfortunate circumstance leads to a severe lethal disease with demise shortly after or before birth; although recognition that some of the respiratory complications are the result of medullary compression has led to more aggressive approach, the outlook for long-term survival has not changed
 Made with Bullet
Made with Bullet