General
- Aka: Lipomyeloschisis
- Should not be confused with myeloschisis which is a severe form of open spinal dysraphism.
Numbers
- Most common closed spinal dysraphisms.
- Lipomyeloschisis + lipomyelomeningocele (rare) account for the majority of all spinal lipomas
Location
- It is most commonly encountered in the thoracolumbar region and usually presents as a fatty subcutaneous mass.
Pathophysiology
- Normal:
- The neural crest converge in the centre to form the neural tube while pulling the ectoderm together in the midline
- Abnormal
- Premature separation of surface ectoderm before the formation of proper neural tube → ingress of mesoderm (which forms fatty elements).
- The mesoderm prevents proper neurulation but closure of the neural tube still occurs so that the meninges and its content is not herniated
Clinical presentation
- Soft, non-tender subcutaneous midline fatty mass just above intergluteal crease
- Cutaneous abnormalities (50%)
- Hypertrichosis
- Atypical dimples
- Acrochordons (pseudo-tails)
- Lipomas
- Haemangiomas
- Aplasia cutis
- Dermoid cyst or sinus
- Most do not have neurological deficit
- Some can present later in life with symptoms of tethered cord
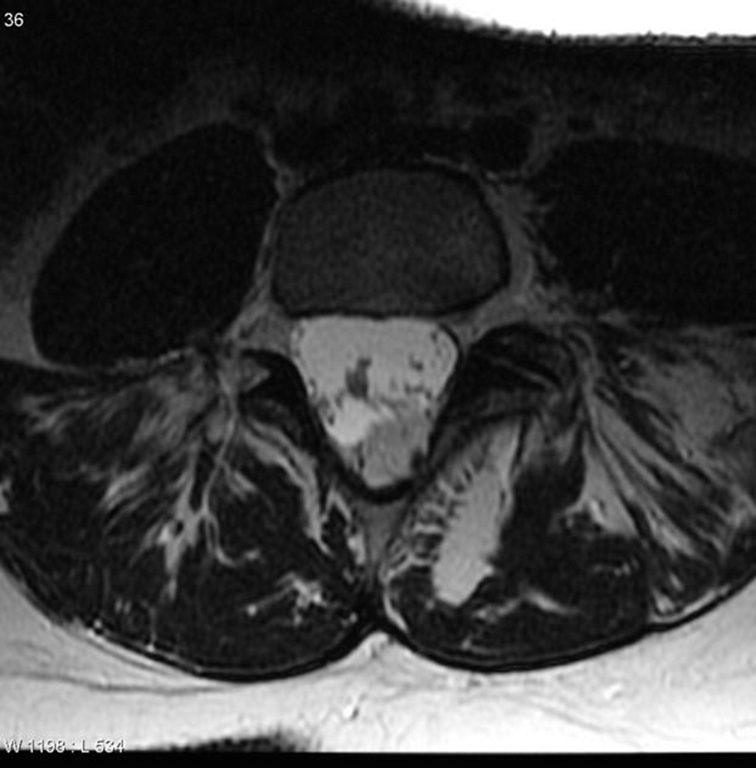
MRI
- Neural placode-lipoma interface lies within the spinal canal or at its edge with normal anterior subarachnoid space.
- There is usually associated tethered low-lying cord or syrinx of the terminal spinal cord.


DDx
Feature | Lipomyelomeningocele | Lipomyelocele |
Definition | Closed neural tube defect with herniation of neural tissue, CSF, and meninges through a dysraphic spine, plus a spinal lipoma contiguous with subcutaneous tissue and attached to dorsal neural placode | Closed spinal dysraphism with lipoma attached to neural placode, neural placode and lipoma remain within the spinal canal without meningeal herniation |
Placode-Lipoma Junction | Lies outside the spinal canal with dorsal extension of meninges through bony defect (meningocele present) | Lies inside the spinal canal; no meningeal herniation beyond spinal canal |
Skin coverage | Intact skin over the lesion | Intact skin over the lesion |
Radiologic findings | Expanded spinal canal, herniation of neural placode, meninges, lipoma; low-lying tethered cord; often with vertebral anomalies | Lipoma and placode identifiable within spinal canal; dilated spinal canal but no herniation of meninges outside canal |
Clinical presentation | Soft tissue mass in lower back, cutaneous stigmata (e.g., hair tuft, dimple), neurological symptoms due to tethering | Similar skin findings but no meningocele; neurological symptoms due to tethered cord possible |
Surgical considerations | Complex due to meningocele and neural involvement outside canal | Less extensive than lipomyelomeningocele, as no meningeal sac herniation |
Common location | Lumbar and lumbosacral region | Lumbar and lumbosacral region |
Embryological basis | Defect in primary neurulation with meningeal protrusion | Defect in neural tube closure without meningeal sac protrusion |
 Made with Bullet
Made with Bullet