Definition
- Congenital fusion of two or more vertebrae.
- This includes C1/2
- Mainly cervical but lumbar and thoracic fusion can occur
Aka
- Vertebral synostosis
Number
- Incidence is 1 in 40,000
- A slight female predominance (3:2).
- Frequently asymptomatic.
Pathophysiology
- Failure of normal segmentation of cervical somites between 3 and 8 weeks’ gestation.
Pathology
- Involved vertebral bodies are often flattened.
- Involved disc spaces are absent or hypoplastic.
- Hemivertebrae may also occur.
- Neural foramina are smaller than normal and oval.
- Cervical stenosis is rare.
- Congenital fusions can occur at any level of the cervical spine
- 75% occur between C1-3.
- The most prevalent fusion is between C2 and C3.
- Iniencephaly
- Complete absence of the posterior elements with an enlarged foramen magnum and fixed hyperextension posture
- Rare.
Concomitant diseases
- Other congenital cervical spine anomalies
- Basilar impression
- Atlantooccipital fusion.
Ranges from
- Fusion of only the bodies (congenital block vertebrae) to
- Fusion of the entire vertebrae (including posterior elements).
Classification
- Type I
- fusion of many cervical and upper thoracic vertebrae,
- Type II
- fusion of 2-3 vertebrae with associated hemivertebrae/occipito-atlantal fusion/other abnormality
- Type III
- cervical fusion with lower thoracic/lumbar vertebral fusion.
Clinical presentation
- Classic clinical triad (all 3 are present in < 50%):
- Low posterior hairline
- Shortened neck (brevicollis)
- Limitation of neck motion
- May not be evident if
- <3 vertebrae are fused
- Fusion is limited only to the lower cervical levels
- Compensated by hypermobility of non-fused segments
- Limitation of movement is more common in rotation than flexion-extension or lateral bending

- Fused segments do not produce neurological deficits
- Symptoms from non-fused segments
- Hypermobile compensation → joint instability or accelerated degenerative arthritic changes.
- Less common in short-segment fusions)
- Other clinical associations:
- Scoliosis in 60%
- Facial asymmetry
- Torticollis
- Webbing of the neck (called pterygium colli when severe)
- Sprengel’s deformity
- 25–35%
- raised scapula due to failure of the scapula to properly descend from its region of formation high in the neck to its normal position about the same time as the Klippel-Feil lesion occurs
- Synkinesis
- Mirror motions, primarily of hands but occasionally arms also
- Less commonly
- facial nerve palsy,
- ptosis,
- cleft or high arched palate.
- Systemic congenital abnormalities may also occur, including:
- Genitourinary (the most frequent being unilateral absence of a kidney)
- Renal USS
- Cardiopulmonary
- CNS
- Deafness in ≈ 30% (due to defective development of the osseous inner ear).
Investigation
- ECG
- CXR
- Foetal US
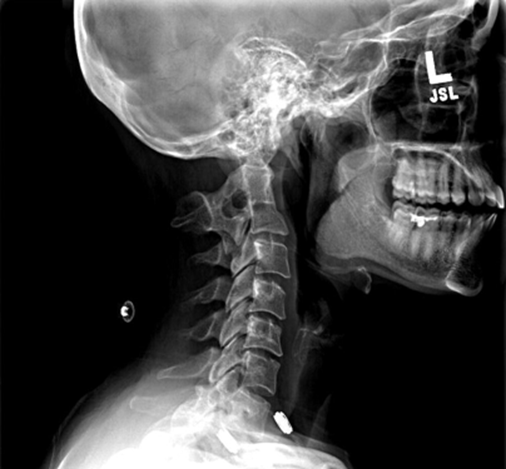
- C spine X ray
- Serial examinations with lateral flexion-extension C-spine X-rays to monitor for instability.
- MRI
- Looking for cord signal change at levels adjacent to the fused segments
Treatment
- Conservative
- Isolated KFS is generally well tolerated
- Initial treatment strategies include modification of activities, bracing, and traction, all of which may delay surgery and prevent neurologic compromise.
- Surgery
- Indication
- Symptomatic instability
- Neurologic compromise
- Cons
- Risk of further loss of mobility
 Made with Bullet
Made with Bullet