Definition
- Marked dilatation of the central canal of the spinal cord, herniating posteriorly through a dorsal spinal defect.
Numbers
- More common in females
- Rare
- 1/400000 births
- No genetic component
- Risk increased with siblings having it
- No nutritional risk factors
Pathology
- Skin-covered mass in the lower lumbar region
- Sac lined by ependyma
Pathophysiology
- A combination of 2 theories
- Cloaca exstrophy → Herniation of the lower part of the abdomen and pelvis → disruption in the secretion by the notochord of inductive factors (normally function to regulate development of the neural tube and regression) → Without the secretion of these factors, the process of secondary neurulation fails to occur.
- Myelocystocele is associated with cloaca exstrophy
- CSF is unable to exit from the early neural tube as it should → mechanical distention of the distal terminal ventricle after canalization → The terminal ventricle then distends the surrounding dorsal membrane and arachnoid, creating the surrounding meningocele.
Clinical presentation
- Skin covered lower lumbar mass
- with or without neurological deficits
Associated abnormalities
- OEIS complex (omphalocele, bladder exstrophy, imperforate anus, and sacral agenesis)
Treatment
- Surgery
- Goal:
- To prevent tethering
- Timing
- Cyst is intact so no rush for surgery
- But should be done within 6 months of age
- Prevent neurological loss from spinal tethering
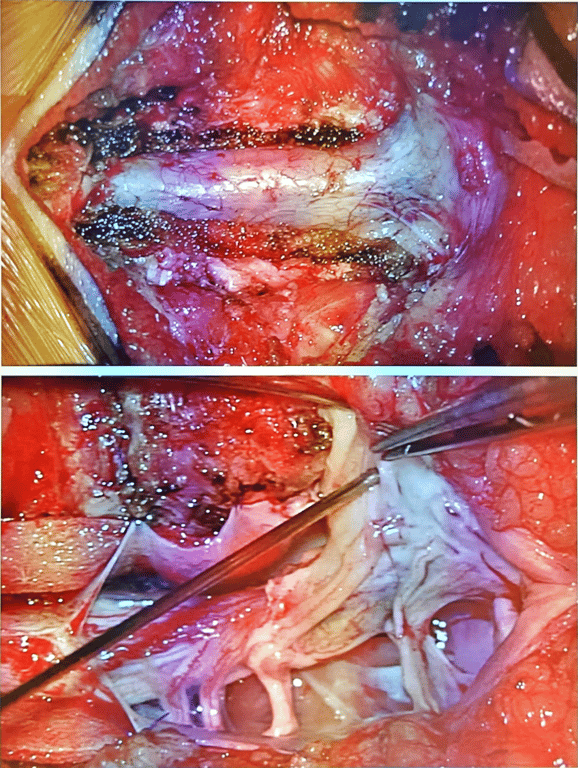
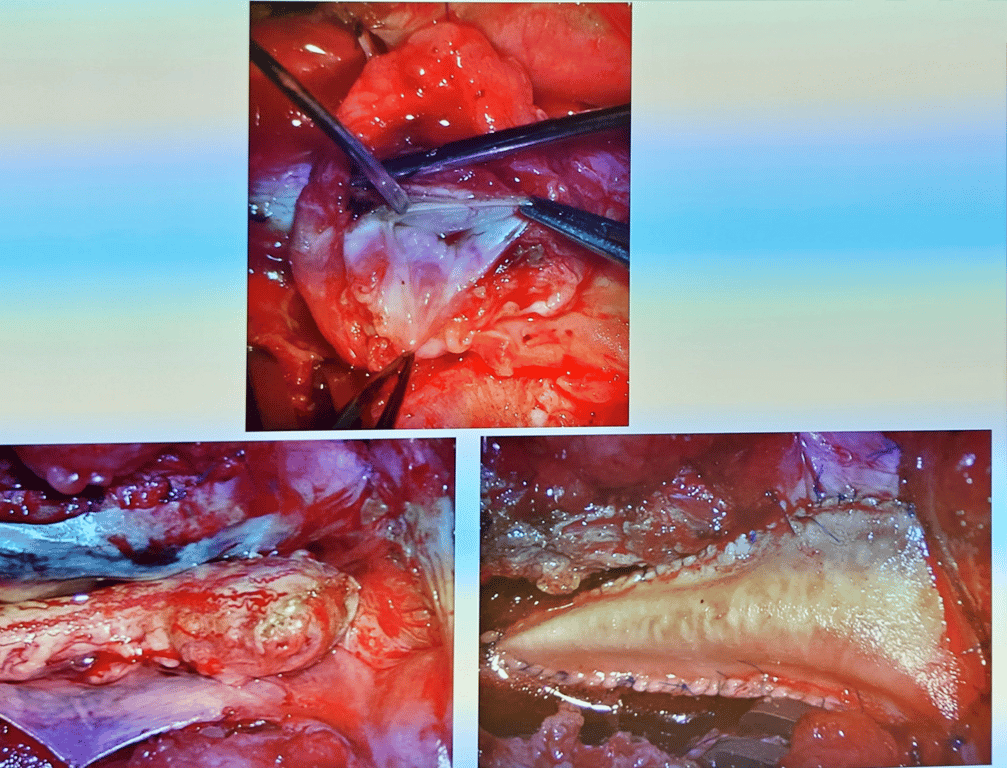
- Images
 Made with Bullet
Made with Bullet