General
- A spectrum of structural defects of the caudal region.
- Malformations vary from isolated partial agenesis of the coccyx to lumbosacral agenesis
Numbers
- Incidence of 1:7500-100000
Aetiology
- Sporadic
- Most
- Familial cases occasionally occur
Associated
- Currarino triad syndromic complexes
- Autosomal dominant: mutations in the MNX1 gene
- Sacral agenesis abnormalities, anorectal malformation and presacral mass consisting of teratoma, anterior sacral meningocele or both
- Maternal diabetes: type I or type II
- 20% of cases of caudal regression syndrome are associated with either type I or type II diabetes mellitus in the mother
- CRS occurs in up to 1% of pregnancies of women with diabetes
- Polyhydramnios
Clinical presentation
- Total or partial agenesis of the spinal column
- Anal imperforation, genital anomalies,
- Neurogenic bladder and anorectal malformations
- Bilateral renal dysplasia or aplasia,
- Pulmonary hypoplasia,
- Sensorimotor paresis (motor deficits > sensory deficits)
- Lower limbs dysplasia, fusion, or agenesis.
- Features of sacral agenesis: narrow hips, hypoplastic gluteal muscles, shallow intergluteal cleft
- Mild foot deformities and gait abnormalities
- 16% of closed spinal dysraphism
Pathology
- Due to failure of secondary neurulation
Radiology
- U/S and MRI
- A blunted sharp ending distal cord on a longitudinal sonogram is typical
- The conus often ends way above the expected level (sometimes even higher than L1)
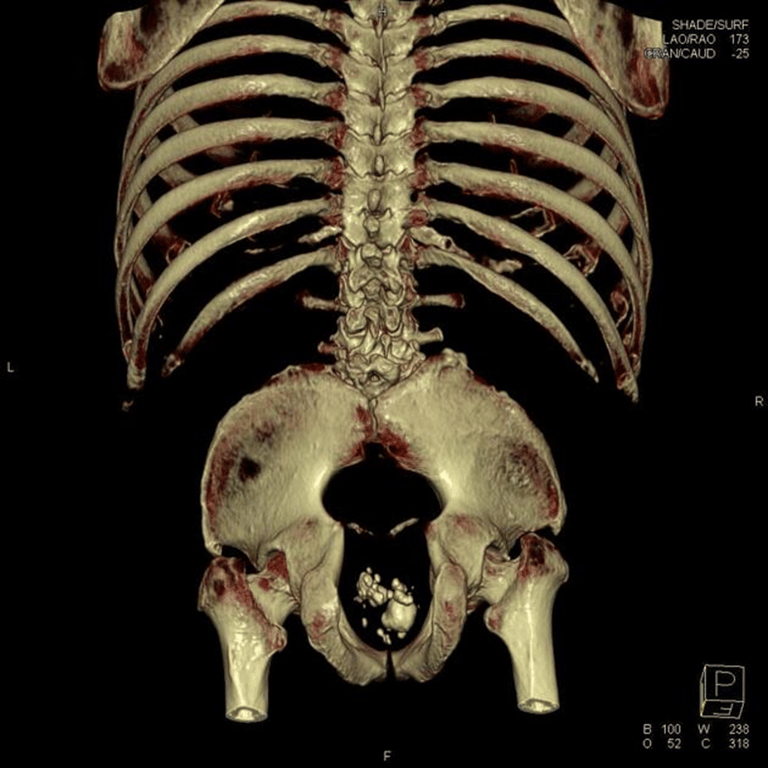
- Absent/hypoplastic sacrum
- Hypoplastic extended lower extremities (limbs are separated cf. sirenomelia)
- May show a "shield sign": opposed iliac bones in absence of sacral vertebrae: typically seen on an axial scan
- Fetal extremities may be seen in a "crossed legged tailor" position or a "Buddha" position
- In an early scan (1st trimester), the crown-rump length may be less than expected for gestational age as an indirect feature


 Made with Bullet
Made with Bullet