General information
- Open fractures tended to occur with MVAs,
- Closed fractures tended to follow accidents at home.
- Dural lacerations are more common in compound fractures.
Number
- Occur in 7-10% of the children admitted to hospital with a head injury.
- 1/3 are closed
- tend to occur in younger children (3.4 ± 4.2 yrs, vs. 8.0 ± 4.5 yrs for compound fractures)
- as a result of the thinner, more deformable skull.
Location
- Most common in frontal and parietal bones.
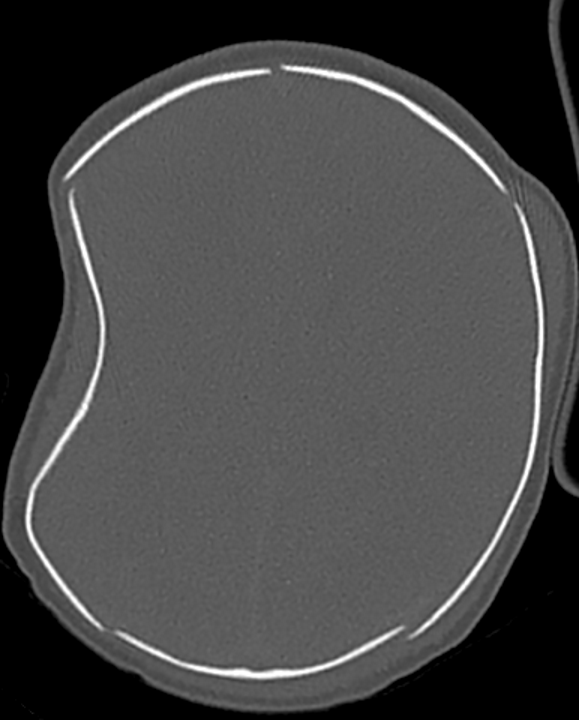
Simple depressed skull fractures
- >1 years old
- deeper the depressed bone (> 1 cm),
- the higher the risk of dural laceration and cortical laceration in adults and older children,
- but less clear in neonate and infant populations.
- Surgical treatment
- Indicated
- fragments are depressed to the depth of at least one thickness of the skull,
- intracranial hematoma,
- dural laceration/CSF leak,
- cosmetically deforming defects,
- gross wound contamination,
- established wound infection.
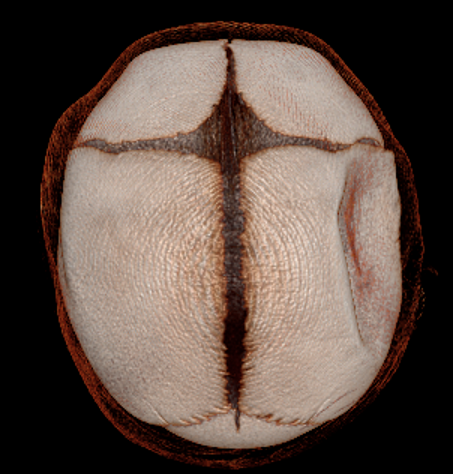
“Ping-pong ball” /Cup shaped fractures
- Depressed skull fractures that occur in children younger than 1 year
- Usually seen only in the newborn due to the plasticity of the skull.
- Commonly after
- Head trauma for post-natal
- Birth trauma for neonates
- A green-stick type of fracture → Outer table is fractured around the periphery, while the inner table fractures at the center → caving in of a focal area of the skull as in a crushed area of a ping pong ball.

Management
- No treatment is necessary when these occur in the temporoparietal region in the absence of underlying brain injury as the deformity will usually correct as the skull grows.
- There was no difference in outcome (seizures, neurologic dysfunction or cosmetic appearance) in surgical vs. nonsurgical treatment in 111 patients < 16 yrs of age.
- In the younger child, remodelling of the skull as a result of brain growth tends to smooth out the deformity.
- Indications for surgery
- radiographic evidence of intraparenchymal bone fragments
- associated neurologic deficit (rare)
- signs of increased intracranial pressure
- signs of CSF leak deep to the galea
- Definite evidence of dural penetration
- situations where the patient will have difficulty getting long-term follow-up
- Persistent cosmetic defect in the older child after the swelling has subsided
- Technique
- Frontally located lesions may be corrected for cosmesis by making a small linear incision behind the hairline, opening the cranium adjacent to the depression, and pushing it back out e.g. with a Penfield #3 dissector.
 Made with Bullet
Made with Bullet