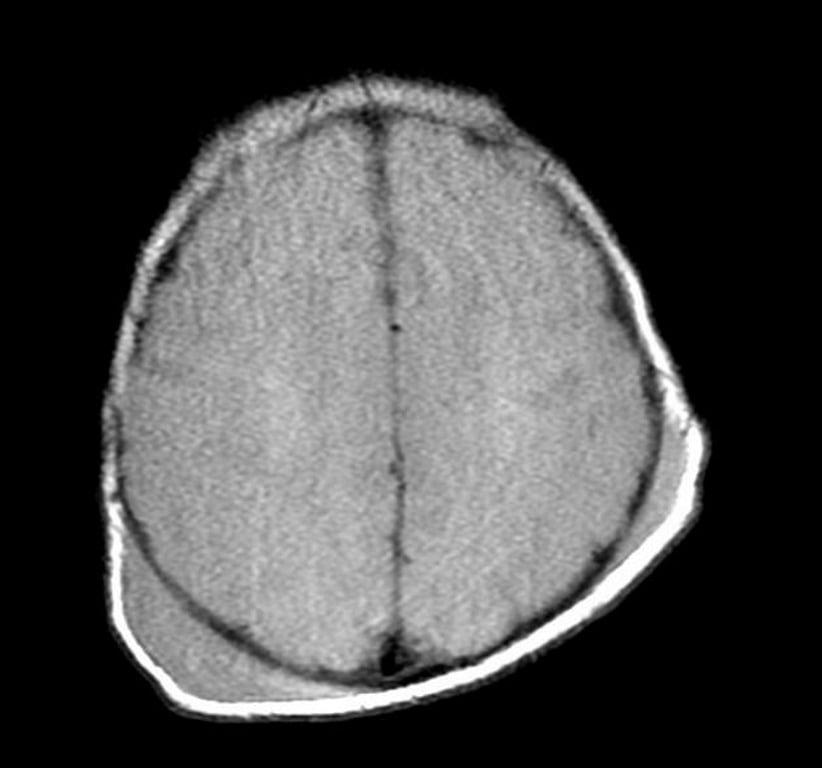
Definition
- Accumulation of blood under the scalp.
- Occurs almost exclusively in children.
Three types:
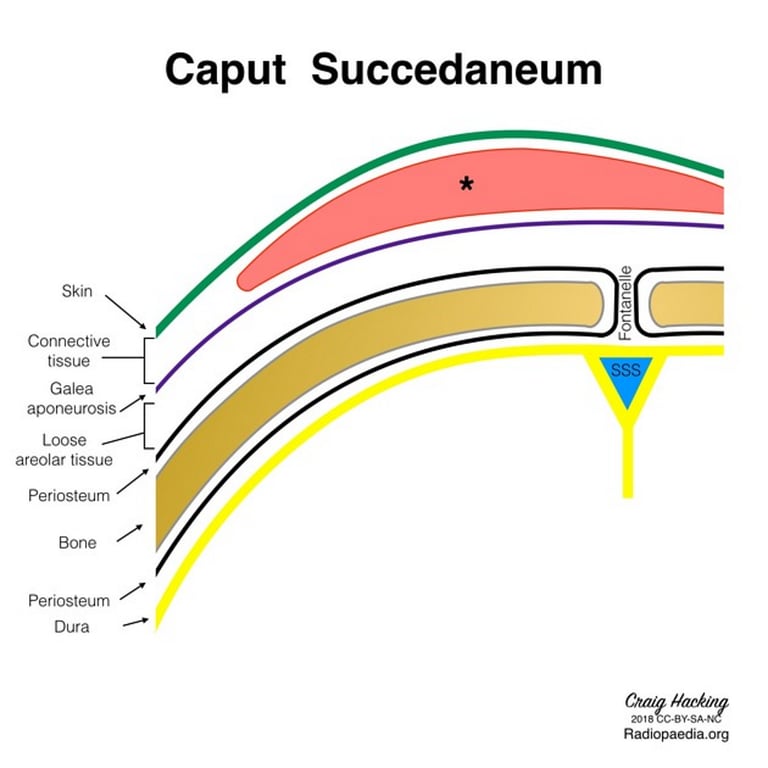
Caput succedaneum
- Clot between skin and galea.
- a manifestation of birth trauma
- The fluid collection is extra-periosteal.
- Pathology
- Results from pressure on the presenting part of the skull against the dilating cervix.
- It extends across the midline and over suture lines and is associated with head moulding.
- Caput succedaneum does not usually cause any complication and usually resolves over the first few days.
- Management is expectant.
Subgaleal hematoma:
- Clot between Galea and periosteum.
- may occur with or without bony trauma,
- linear nondisplaced skull fracture (especially in age < 1 yr).
- Pathology
- May cross sutures.
- Usually starts as a small localized hematoma, and may become huge (with significant loss of circulating blood volume in age < 1 year, transfusion may be necessary).
- Inexperienced clinicians may suspect CSF collection under the scalp which does not occur. Usually presents as a soft, fluctuant mass.
- These do not calcify


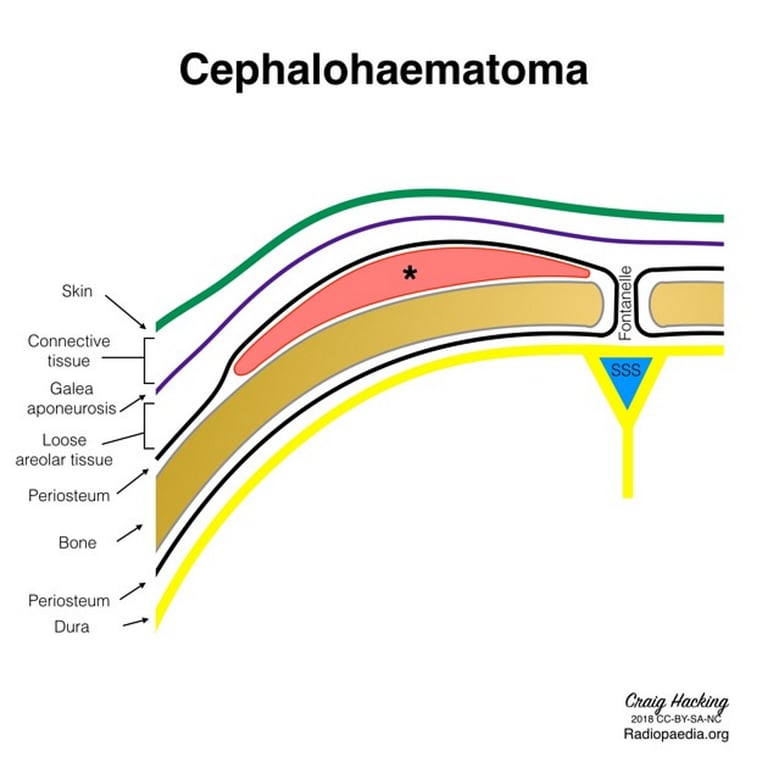
Subperiosteal hematoma
- Clot between Periosteum and bone
- Aka cephalhematoma
- Most commonly seen in the newborn
- Associated with
- Parturition (giving birth)
- Neonatal scalp monitor
- Bleeding elevates periosteum, extent is limited by sutures.
- Firmer and less ballotable than subgaleal hematoma;
- scalp moves freely over the mass.
- 80% reabsorb, usually within 2–3 weeks.
- Occasionally may calcify

For all cases
- Infants may develop jaundice (hyperbilirubinemia) as blood is resorbed, occasionally as late as 10 days after onset.
Treatment
- Treatment beyond analgesics is almost never required, and most usually resolve within 2–4 weeks.
- Ensure Vit K is given and check clotting and FBC.
- Avoid the temptation of percutaneously aspirating these because the risk of infection exceeds the risk of following them expectantly, and in the newborn removal of the blood may make them anaemic.
- Follow serial haemoglobin and haematocrit in large lesions.
- If a subperiosteal hematoma persists > 6 weeks, obtain a skull film.
- If the lesion is calcified, surgical removal may be indicated for cosmetic reasons (although with most of these the skull will return to normal contour in 3–6 months)
 Made with Bullet
Made with Bullet