Untreated adolescent idiopathic scoliosis in the adult
Degenerative changes Iatrogenic Paralytic
Age of Presentation
Patients generally have known about their scoliosis for decades.
Generally presents in the 6th decade of life.
Curve pattern
Follows classic curve patterns
Lack classic curve patterns
Vertebral segments
Involves more vertebral segments.
Involves fewer vertebral segments
Curve location
Thoracic spine. Sometime involve the lumbar spine
Lumbar spine (apex is usually L3). Often does not involve the upper thoracic spine.
Curve magnitude
Larger curves
Smaller curve magnitude
Associated Curves
N/A (Focus is on the persistence of the original adolescent curve).
Frequently involves a compensatory curve from T11 to L2 and a fractional curve from L4 to S1.
Symptom Characteristics
May or may not be painful, but it is usually not disabling. Patients typically present when back pain becomes more disabling or when radiculopathy worsens.
Does not always cause midline, axial back pain. Many adults are unaware they have scoliosis until a radiograph reveals it.
Specific Associated Pathologies
Presentation often includes worsening radiculopathy.
Frequently manifests as radiculopathy due to lateral recess stenosis, foraminal stenosis, lateral olisthesis, or spondylolisthesis. As it worsens, it may be accompanied by L3–4 lateral olisthesis and L4–5 spondylolisthesis.
Treatment Considerations
Curve magnitude in and of itself is usually not an indication for surgery. Cardiopulmonary compromise is generally not a concern once a patient stops growing, unless the Cobb angle exceeds 70°.
Treatment often focuses on alleviating neurogenic pain or stabilizing instability (e.g., L3–4 lateral olisthesis), potentially using focal treatments to target pain generators.
Fractional curve: The minor curve below the major curve
European Spine Study Group (ESSG) and International Spine Study Group (ISSG) databases: (Ames 2019)
Unsupervised hierarchical clustering (AI)
Data patterns may augment preoperative decision making: risk vs benefit of surgery
Degenerative spinal changes and sagittal malalignment
Muscular dystrophy, camptocormia, osteoporosis
Secondary postoperative deformity
Three-dimensional:
De novo scoliosis
Degenerative scoliosis
Neuromuscular, Parkinson
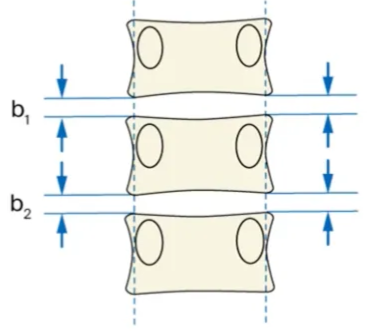
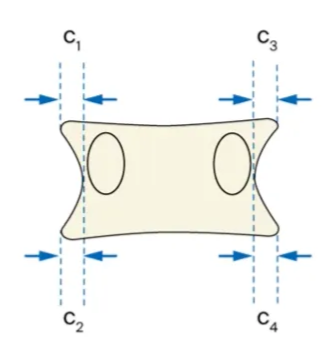
Pathophysiology
Asymmetric disc and facet joint degeneration:
The process often begins with degeneration of the intervertebral discs and/or facet joints, which occurs unevenly on either side of the spine.
This asymmetric breakdown leads to abnormal loading in specific spinal segments.
Vicious cycle of deformity progression:
The resulting asymmetric loading furthers the degeneration, leading to a self-perpetuating “vicious cycle.”
As the structural integrity of the vertebrae, discs, and facet joints worsens, the spinal curve (scoliosis and/or kyphosis) progresses.
Instability:
Destruction of the discs, facet joints, and joint capsules causes instability, both in the sagittal and frontal planes.
This instability can be segmental (affecting specific segments) or multisegmental, ultimately leading to spondylolisthesis (slippage) or rotational/translational dislocations.
Osteophyte formation and ligamentous changes:
The body attempts to compensate for instability with the formation of osteophytes (bone spurs) on the facet joints and vertebral endplates.
Ligamentum flavum and joint capsules also thicken and may calcify, further narrowing the spinal canal and contributing to central and foraminal (lateral) spinal stenosis.
Role of osteoporosis:
In postmenopausal women especially, reduced bone density (osteoporosis) increases the risk for asymmetric vertebral collapse, amplifying progression of the scoliotic curve.
Muscular imbalance and pain:
The abnormal spinal alignment overloads certain musculature, particularly the paraspinal muscles.
Chronic muscular fatigue and pain further reduce spinal stability and functional compensation, worsening the deformity.
Associated with
Disk degeneration
Facet arthritis
Thickening/hypertrophy of the ligamentum flava
Loss of lumbar lordosis
Lateral listhesis
Stoke's Vicious Cycle of Pathogenesis:
Type 2 adult scoliosis
General
Idiopathic adolescent scoliosis → into Adulthood (AdIS)
Progression due to mechanical reasons or bony and/or degenerative changes
Unlike the paediatric patients, adult patients present with
Pain
Radicular symptoms.
Mortality rate of untreated adult patients with adolescent idiopathic scoliosis is comparable with that of the general population
Coronal deformity linked to leg-length discrepancy
Three-dimensional:
Early onset scoliosis (EOS) at skeletal maturity
Adolescent idiopathic scoliosis (AIS) at skeletal maturity
Congenital scoliosis
Neuromuscular or syndromic scoliosis
Progression of deformity over time: Degenerative change and curve progression in adolescent idiopathic scoliosis
As young adults
Clinical trunk imbalance
Mainly self-image altered
Low-level of functional impairment
Progression risk during adulthood
In adulthood
Lumbar curve dislocation
Increase in trunk asymmetry
Coronal and sagittal malalignment
Degenerative lumbar changes
Surgery
Fusion levels
For thoracic and lumbar curves
>35 deg and graded as structural require them to be included in the arthrodesis
Non structural curve < 30 deg can be excluded from the fusion.
Fusion of Lumbar sacral cruves
depends on
Presence of radiculopathy
Age
Bone density
presence of significant degeneration on MRI
Type 3 adult scoliosis
Aka secondary adult scoliosis
Subtype
3a Due to pelvic obliquity
Eg: leg length discrepancy, hip pathology, etc.
Most located at thoracolumbar, lumbar-sacral
3b Due to metabolic bone disease
Eg: osteoporosis + arthritic disease/fractures; Metabolic bone disease
Natural history
Curves < 30° generally do not progress,
Curves 30-50° progress 10-15° during life
Curves 50-75° progress at 1° per year.
Curve progression rates depending on Initial angle and bone quality.
Importance of curve progression as a symptom and predictor.
Clinical features
---
title: Assessment of adult deformity
---
flowchart TD
%% Main Complaint, branching first
subgraph MC["Main Complaint"]
C3["Disability"]
C2["Radiculopathy"]
C1["Back Pain"]
C4["Neurogenic<br>claudication"]
end
%% Disability branch (leftmost, no cross)
C3 --> D3["Assess level and kind<br>of disability"]
%% Radiculopathy branch (left-mid)
C2 --> D2["Correlate with imaging<br>findings and injection<br>confirmation"]
D2 --> n1["Consider lateral recess<br>or foramen stenosis"]
%% Back Pain branch (center/main stem)
C1 --> D1["Back Pain Location"]
D1 --> E2["Paraspinal"]
D1 --> E1["Midline Lumbar"]
%% Midline branch (above, more central)
E1 --> F1["Position Dependence"]
F1 --> G2["Relentless, no<br>position relief"]
G2 --> H2["Treat as chronic<br>low back pain"]
H2 --> H3["Consider psychological<br>profile and 2nd gain"]
F1 --> G1["Pain worsens upright,<br>relieves supine"]
G1 --> H1["Consider scoliosis or<br>imbalance as pain<br>generator"]
H1 --> H4["Radiology assessment:<br>Roussouly type,<br>Presence of Olisthesis,<br>Spino-pelvic parameters,<br>Pelvic incidence,<br>lumbar lordosis mismatch,<br>Increased compensatory pelvic tilt,<br>Pathologic SVA<br>(Age-appropriate threshold),<br>Pathologic CVA"]
%% Paraspinal branch leads to radiculopathy node so is grouped
E2 --> D2
%% Neurogenic claudication, rightmost, no cross
C4 --> n2["Correlate with imaging<br>findings and injection<br>confirmation"]
n2 --> n3["Consider central canal<br>stenosis"]
Symptoms
Low back pain
Commonest symptom (40-90%)
Patients with scoliosis have an incidence of low back pain similar to the general population.
Character
Axial
more diffuse and generalised
Mechanical or non mechanical
worse or independent with activity
relief with lying
some patients might feel pain is better with walking
walking may paradoxically improve the symptoms because the forward propulsion of the body may allow some compensation for the forward leaning in cases of positive SVA
Exacerbated by certain postures
More severe and recurrent than general population
At curve apex, concavity, countercurve.
Importance of axial loading and postural influence (pain relieved by lying down).
Caused by
Spondylosis
Micro/macro instability
Discogenic pain
Evaluation of pain source
Discography
Neuro-foramen imaging
Computed tomographic myelography:
Foraminal stenosis or lateral nerve-root compression
Selective nerve root block
Precise segmental localization diagnosis
Diagnosis: lidocaine (0.5%)
Treatment: dexamethasone
Indications:
Lumbar disc herniation
Lumbar spinal stenosis
Degenerative scoliosis
Lumbar spondylolisthesis
Differentiating Scoliosis-Related Pain from Chronic Pain
Scoliosis-Associated Pain:
Pain is typically exacerbated in an upright position (e.g., standing or walking).
The pain is usually alleviated when sitting or lying down (unloading the curved spine).
Painful scoliosis usually worsens progressively over years.
Chronic Low Back Pain (Unrelated to Scoliosis):
If the pain is midline and relentless regardless of position or activity
In these cases, consideration of the patient's psychological profile and secondary gain (any external or indirect benefit a person receives from their symptoms, illness, or disability) is important, as surgery may not be beneficial.
Location of pain (midline vs paraspinal)
Two types
Midline tend not to be scoliotic pain
Paraspinal tend to be radicular and neurogenic claudication
Assessments are used to identify nerve compression:
Radiological correlation:
MRI, CT to identify if stenosis in the lateral recesses or foramina is causing nerve compression.
Radicular vs. Paraspinal Manifestation:
Although there may be nerve compression, the radiculopathy might manifest only as paraspinal back pain, without radiating down the lower extremities.
Diagnostic Injections:
In patients with multilevel stenosis or ambiguous symptoms, a selective nerve root block or transforaminal epidural injection can help clarify whether the stenosis is the source of the pain.
Temporary alleviation of pain following the injection can confirm the pain generator, indicating a potential target for focal surgical treatment.
Assessment of other pain sources
Facet-Mediated Pain:
This pain causes paraspinal symptoms and can be tested using medial branch blocks.
Sacroiliac (SI) Joint Pain:
This contribution is evaluated through clinical examination and diagnostic sacroiliac joint injections.
Olisthesis:
The presence of lateral olisthesis itself is associated with increased disability, and the pain may originate solely from the olisthesis rather than the entire scoliosis.
Muscular Pain:
Evaluation should consider pain in the paraspinal musculature due to fatigue from maintaining upright posture in the setting of sagittal plane imbalance.
Greater trochanteric pain syndrome:
Also commonly seen in patients with degenerative lumbar pathologies.
Neurological deficits
Due to
Segmental instability
Foraminal compression
Congenital spinal stenosis
Severe canal stenosis
Neurogenic pain
Can manifest in two main ways:
Classic Neurogenic Claudication: (60%)
Pain in lower extremities and buttocks
Unlike classic claudication, patients with scoliosis + stenosis do not obtain relief with sitting / forward flexion
Stenosis is located on the concave side of the curve
70% of central stenosis occurred at the junction between the lumbar and lumbosacral curves
Rotational subluxation
L3/4 most common
At lumbar/lumbar sacral curve junction
Paraspinal Radiculopathy Without Radiation:
This is nerve pain that manifests as paraspinal back pain rather than radiating down the legs.
Location of pain (midline vs paraspinal)
Two types
Midline tend not to be scoliotic pain
Paraspinal tend to be radicular and neurogenic claudication
Assessments are used to identify nerve compression:
Radiological correlation:
MRI, CT to identify if stenosis in the lateral recesses or foramina is causing nerve compression.
Radicular vs. Paraspinal Manifestation:
Although there may be nerve compression, the radiculopathy might manifest only as paraspinal back pain, without radiating down the lower extremities.
Diagnostic Injections:
In patients with multilevel stenosis or ambiguous symptoms, a selective nerve root block or transforaminal epidural injection can help clarify whether the stenosis is the source of the pain.
Temporary alleviation of pain following the injection can confirm the pain generator, indicating a potential target for focal surgical treatment.
Radicular symptoms
in the form of (all derma/myotomal)
Leg pain
Leg weakness
Leg numbness
Caused by
Foraminal and lateral recess stenosis
Worse in concavity of the deformity where there is vertebral body rotation and translation
Prevalence of concurrent significant cervical cord compression in patients with ASD is relatively high at 33.8%
increased risk of cervical cord compression in
Older age
Increased BMI
High PI-LL mismatch
Clinical assessment
Physical exam
Skin
Neurocutaneous syndrome
Muscle
Bulk/tone asymmetrical
Weakness
Gait and posture
Assessment of stability
Patients may be considered clinically balanced—even if radiographic discordance exists—if they state they have no problems standing up straight and clinically stand straight with normal hip and knee extension.
Malalignment
trunk shift
forward/lateral bending test
Deformity with thoracic prominence seen with forward bending
Asymmetry of shoulder and pelvic girdle
hip and knee flexion contractures
Flexibility of curve in prone positioning
Hip/knee flexion
Forward trunk inclination
Posterior pelvic tilt
Horizontal gaze
Dorsiflexion of ankle during walking
Camptocormia
An axial muscle myopathy associated with Parkinson’s disease.
Be wary of the adult deformity patient whose deformity appears when they stand or walk, but disappears when they lie down.
Provocative testing
Helps to elucidate the pain generators:
Facet/nerve root blocks
Discograms
Aims:
To determine the necessary portions of pathology that should be addressed, would best relieve the patient’s symptoms, and produce a successful clinical outcome.
Deformity assessment
Check patient’s spinal shape from the back and the sides.
Pathologic Sagittal Vertical Axis (SVA) (taking into account age-appropriate thresholds).
Pathologic Coronal Vertical Axis (CVA).
Other assessment
Pelvic Obliquity
Pelvic coronal reference line (PCRL):
Tips or sulcus of the sacral ala OR
Alternatively, the top of the ilium may be used to create the PCRL.
An angle between PCRL and a horizontal reference line is then measured
Leg length discrepancy (LLD)
Measured using PA standing radiographs without blocks under the patient’s feet and with the knees extended.
A femoral horizontal reference line (FHRL) a horizontal line that is tangent
to the top of the highest femoral head OR
to the level of the lesser trochanter.
The difference between the height of this line and the height of the lower femoral head is then measured as the LLD.
interpretation
If the left hip is up, the value is positive (+).
If the right hip is up, then the value will be negative (−).
Poorer clinical outcomes have been associated with
Sagittal (C7-SVA, PT, LL, sagittal LIVDA) and/or
Coronal imbalance (C7-CSVL, shoulder-tilt, and pelvic obliquity).
Clavicle angle
Angle between
Line connecting a the highest points of the clavicles
drawn perpendicular to the lateral edge of the radiograph and touches the most cephalad portion of the elevated clavicle and a line which touches the most cephalad aspect of both the right and left clavicles (clavicle reference line)
Horizontal plane
Angles in which the left shoulder up are positive
Angles with the right shoulder up are negative.
This directionality is consistent with that of the T1 tilt angle described earlier.
Clavicle tilt has been shown in some studies to have an association with postoperative shoulder imbalance
In the future more people will require deformity surgery
Due to aging population
Need to have good patient selection
Patient must have realistic goals
Patient must have awareness of the significant potential for complications
Medical comorbidities may mean that some patients are not fit enough for the magnitude of surgery that is required.
In many cases the choice is to do nothing or a small decompressive procedure, or to consider a bigger operation and correction of the deformity, a procedure which will usually require an osteotomy or multiple intervertebral cages.
A simple decompression (leaving the deformity uncorrected) may relieve radicular symptoms, but a ‘small fusion’ may leave the patient in a worse sate, if the problems of lost lordosis and global spinal balance are not addressed.
If the deformity is to be addressed, then the correction goals are restoration of the patient’s sagittal vertebral alignment.
Continuum of Care: Nonoperative management exists on a continuum with operative treatment, with a "grey zone" where various modalities like physiotherapy, pain management, and injections are employed.
Nonoperative
Indications
Coronal curves < 30 degrees rarely progress
Deformity surgery does not prevent progression of deformity
Patient choice: When patients are unable to undergo or do not want surgery.
Technical factors.
Even if surgery is not an option, patients still need treatment to manage pain and maintain mobility.
Pros of Nonoperative Management:
Reduces pain and improves mobility for patients who cannot or do not want surgery.
Statistically, it can show no difference in global outcome measures compared to operative treatment.
Avoids surgical risks and lengthy rehabilitation.
Can prevent progression in skeletally immature patients.
Provides time to understand patient expectations and optimize the patient ("prehabilitation").
Cons of Nonoperative Management:
Does not treat the causative problem.
Can delay time-to-surgery in undecided patients.
In adults, it generally does not prevent progression of deformity or neurological compromise.
Palliates symptoms over a reduced period of time.
Requires adherence, understanding, and sacrifice from the patient.
Less effective in small, nonprogressive, or mature curves.
Modalities:
Active Therapies: Require patient participation.
Physical therapy: Includes exercise-based approaches to increase flexibility, build strength and endurance, improve core strength, postural training, activity modification, weight management, and bracing. Benefits include improved flexibility, strength, muscle tone, stiffness relief, better balance/coordination/sleep, cardiovascular stimulation, and pain improvement.
Neuromuscular reeducation.
Functional restoration program (including psychosocial counseling).
The GLA:D (Good Life with osteoArthritis: Denmark) program is an example of a neuromuscular exercise program for osteoarthritis that can be done at home.
Passive Therapies: Do not require patient participation.
Physical modalities: Massage therapy, transcutaneous electrical nerve stimulation (TENS), hot/cold packs, therapeutic ultrasound. Benefits include reducing muscle spasm, managing pain pathways, and reeducating patient response to pain.
Bracing
No role in adult deformity
Does not slow progression
Might help with pain but can decondition the patient
Include nerve-root blocks, caudal epidural, trigger point injections, and radiofrequency ablation (RFA).
These can be diagnostic (to identify pain origin) or therapeutic, have minimal side effects, and can be repeated up to twice yearly, though efficacy may decrease over time.
Performed under image guidance (intensification/ultrasound/CT/MRI).
Alternative/allied medicine: Chiropractic/osteopathic manipulation, massage, and stretching techniques.
Operative
Treatment Goals
To Balance the Spine
Addressing Sagittal Imbalance (SVA):
If a patient has a positive SVA and appears forward leaning, but states this position is not disabling and only wants their neurogenic symptoms resolved, the goal may not be to balance the spine.
Addressing Coronal Imbalance:
Coronal imbalance is generally defined as a shift of 3 or 4 cm in the C7 plumb line relative to the central sacral vertical line.
However, treatment may not be necessary if the patient does not find the imbalance self-apparent or symptomatic.
To Treat Neurogenic Pain
To Treat Back Pain Originating from the Scoliosis
General Considerations
Operative
treatment can be superior to nonoperative care for some patients.
Pros:
Decompresses neural structures (radicular pain),
Stabilizes the spine (curve progression, segmental rotatory instability)
Associated with complications, may necessitate reintervention, and incurs costs.
Surgery can be cost-efficient at 10 years if no complications occur.
However, reoperation rates are significant, ranging from >20–30% at 2 years.
Pellise 2024: Complications and reoperations are considered unsustainable in value-based healthcare, reducing surgical gains (QALYs), decreasing gains by 40% with every revision surgery, increasing patient morbidity and mortality, and increasing overall costs.
Decisions involve a pathway that considers increasing invasiveness/aggressiveness:
Decompression (no fusion): Primarily for radicular pain that is greater than axial pain, in cases with a stable spine and little deformity without sagittal malalignment.
Stabilization (short fusion): For cases where radicular pain equals axial pain, segmental instability is present, and there is little deformity without sagittal malalignment.
Deformity Correction (long fusion): Primarily for axial pain and sagittal malalignment.
When the patient's back pain is genuinely related to the scoliosis itself
Differentiating Scoliosis-Related Pain from Chronic Pain
Scoliosis-Associated Pain:
Pain is typically exacerbated in an upright position (e.g., standing or walking).
The pain is usually alleviated when sitting or lying down (unloading the curved spine).
Painful scoliosis usually worsens progressively over years.
Chronic Low Back Pain (Unrelated to Scoliosis):
If the pain is midline and relentless regardless of position or activity
In these cases, consideration of the patient's psychological profile and secondary gain (any external or indirect benefit a person receives from their symptoms, illness, or disability) is important, as surgery may not be beneficial.
Deformity and Imbalance: AND
To correct symptomatic sagittal or coronal imbalance.
To measure and correct
Roussouly type
Presence of Olisthesis
Spino-pelvic parameters
Pelvic incidence-lumbar lordosis mismatch
Increased compensatory pelvic tilt
Pathologic Sagittal Vertical Axis (SVA) (taking into account age-appropriate thresholds).
Pathologic Coronal Vertical Axis (CVA).
Severe Multilevel Pathology: AND
In cases of severe, multilevel degeneration with resultant stenosis that cannot be addressed with focal decompression and fusion.
This includes patients with:
Stenosis extending from L1 to S1 or L2 to L5.
Lumbar stenosis with concomitant L4–5 spondylolisthesis, L3–4 lateral olisthesis with stenosis, or degenerative changes at L1–2 or higher.
Extensive Decompression Requirement: When a multilevel laminectomy is necessary for multilevel stenosis, the inherent destabilizing nature of extensive decompression mandates instrumented fusion.
Extension of the Fusion to the Upper Thoracic Spine (Above T10, generally T2-T4)
Aim is
To prevent mechanical failure
Adequately correct global deformity
Indications:
Thoracic Deformity:
In cases of sweeping thoracolumbar scoliosis where fusion to T10 will not encompass the entire Cobb angle of the scoliosis.
Severe Kyphosis:
When there is significant thoracic kyphosis.
Sagittal Balance/Kyphotic Apex:
If fusion stopping at T10 is at or near a kyphotic apex, or if stopping at T10 will not restore the patient’s SVA.
Proximal Junctional Kyphosis (PJK) Risk:
To mitigate PJK risk, especially when substantial correction is planned:
When correction of the SVA at T10 will predictably result in PJK.
If the patient has a hyperlordotic T10 or a kyphotic T8–10 angle.
If the patient has a thoracic kyphosis of 30° or more and is undergoing induction of lumbar lordosis of 30° or more.
Severe Deformity/Osteotomy:
In patients with greater deformities who undergo three-column osteotomies, fusion to the upper thoracic spine may provide better correction and lower PJK rates than fusion to the lower thoracic spine.
Note:
Studies suggest that fusion to the upper thoracic spine does not necessarily improve outcomes or correction compared with fusion to the lower thoracic spine, and upper thoracic fusion is associated with higher total complication rates, more blood loss, and longer operative times. Therefore, T10 is often preferred unless the high-risk factors above mandate a more cranial endpoint.
Stopping the Fusion Below T10 (in the Lumbar Spine)
Fusion can sometimes terminate in the lumbar spine when the primary problem is focal neurogenic pain, and the scoliosis is less concerning for global imbalance.
Indications:
Primary Symptom:
When patients mainly present with neurogenic claudication secondary to lumbar stenosis but also have concomitant scoliosis.
Structural Integrity:
If there is no olisthesis or significant rotation at the chosen UIV, and no junctional kyphosis is present at the UIV.
Relationship to UEV:
The UIV should generally be cephalad to the Upper End Vertebra (UEV) of the scoliosis.
Absence of Thoracic Deformity:
If patients do not have thoracic kyphosis or kyphosis at the thoracolumbar junction, placing the UIV at L1 was found to have no difference in PJK incidence compared to higher levels.
Note:
Curve Apex Avoidance:
The UIV should be away from the apex of the scoliosis.
Decreased Reoperation Risk:
In patients fused to the sacrum, a UIV in the lumbar spine had a lower rate of reoperation than a UIV in the thoracic spine.
A lower UIV, reduces blood loss and operative time
Limited Fusion or Even Decompression Only
Limited, focal treatment is preferred when the primary source of disability is localized pathology rather than the global scoliotic curve.
Indications:
Focal Pain Generator:
When a focal source of pain (such as nerve compression, spondylolisthesis, or lateral olisthesis) can be identified as the source of disability, and the patient is otherwise well-balanced.
No radiographic evidence of instability
Specific Stenosis Type:
Decompression only (e.g., laminotomy) may be suitable if the main compression is dorsal-ventral (due to ligamentous and facet hypertrophy).
Comorbidity Consideration:
Limited surgical extension may be considered for patients with significant comorbidities who cannot tolerate extensive surgery.
Note
Limited Fusion of Concavity: Can be used when radiculopathy is strictly referable to the concavity of the scoliosis, and there is no back pain.
Caution for Decompression Only: can fail and patients should be counseled about the potential need for eventual fusion. It is critical to maintain stability by avoiding a complete laminectomy.
Decompression alone is not recommended for severe up-down foraminal stenosis where interbody fusion is a better option for stabilization and alleviation.
Fractional Curve Fusion Only
Fractional curve
The minor curve below the major curve.
Location:
Typically found from L4 to S1.
Sometimes, the symptomatic level within this curve may involve only L5–S1.
Clinical Significance:
Although it is the minor curve, the fractional curve can be a significant source of pain.
Pathology:
Degeneration of the fractional curve may lead to severe lumbar stenosis, spondylolisthesis, and up-down (foraminal height) foraminal stenosis, which can cause disabling pain.
Upright scoliosis radiographs are considered critical for assessing the lumbosacral fractional curve, as many patients present with radiculopathy caused by up-down foraminal stenosis on the concavity of this curve when axial loading occurs.
Aim
Treatment of the fractional curve only has demonstrated good outcomes when the goal is to resolve radicular pain, even if long-standing chronic low back pain persists.
Indications for Fractional Curve Fusion Only:
Primary Symptom:
When the fractional curve is the significant source of disabling pain, and the pain is radicular in nature and referable to that curve.
Pathology:
When degeneration of the fractional curve causes severe lumbar stenosis, spondylolisthesis, and up-down foraminal stenosis.
Specific Level Pain:
If the symptomatic level involves only L5–S1.
Note
Extension Consideration:
If there is lateral olisthesis at L3–4, one should consider including L3–4 in the fusion construct to address the olisthesis, rather than strictly limiting the fusion to the L4–S1 fractional curve.
Interbody Fusion:
Interbody fusion is often a useful option here, as increasing disc height can alleviate up-down stenosis.
Coronal Caution for Nanjing C or Obeid 2: as correcting the fractional curve alone can lead to worsening coronal alignment.
Correction vs fusion in situ
Approach
Indication
Goal
Pros
Cons
Correction
Severe, unbalanced, progressive curves
Restore alignment
Improved balance, less pain from deformity
Higher risk, more invasive
Fusion in situ
Non-progressive, balanced deformity
Stabilize without correction
Low complication rate, good for frail/elderly
No alignment change, may not relieve all symptoms
Correction (Surgical Realignment)
Goal:
Actively restore normal spinal alignment (both in the coronal and sagittal planes) by manipulating and correcting the curve during surgery.
Indications:
Significant malalignment,
Severe pain,
Progressive deformity, or
Sagittal/coronal imbalance that impairs function or quality of life.
Method: Surgical techniques include osteotomies, anterior or posterior release, use of instrumentation (rods, screws) to realign and fix the spine in a more anatomical position.
Technique
Short segment decompression +/- fusion
Indication
Presence of nerve root compression AND
Sagittal plane is balanced (avoid doing short segment if patient has sagittal malalignment)
Young pt (40-60 yrs) preserve lumbar spine flexibility
Elderly patient with lumbar canal stenosis
Deformity surgery
Indications
Curve > 50 degrees of the following type
Thoracic curves >60deg affect pulmonary function tests
Thoracic curves >90deg affect mortality
Sagittal imbalance
Curves progress
Cobb > 10° AND/OR
Increase in subluxation > 3 mm
Increasing clinical symptomatology
Intractable back pain or radicular pain that has failed nonsurgical efforts
Long segment decompression required
Cosmesis (controversial)
Signs of radiological progression risk factor as above
posterior only curve correction and instrumented fusion
indications
thoracic curves > 50 degrees
most double structural curves > 50 degrees
selecting technique is patient and surgeon specific
combined anterior/posterior curve correction with instrumented fusion
Improved spinal balance → potential reduction in compensatory mechanisms (e.g., pelvic tilt, knee flexion) → relief from pain caused by malalignment.
Risks:
Greater surgical time, increased risk of complications (blood loss, neurological, infection), higher demands on bone quality, especially in elderly or osteoporotic patients. May not be appropriate in frail or high-risk individuals.
Aebi's Emphasis: Carefully selected patients benefit most from correction, particularly if the deformity is rigid or unbalanced and if there is risk for further progression or functional decline.
Fusion In Situ (Accepting Balanced Deformities)
Goal:
Fuse the spine as it is, without attempting major realignment, provided that the patient is already balanced in sagittal and coronal planes
Fusion is performed at the necessary levels to stop progression or stabilize symptomatic segments, often involving less extensive surgery, with or without instrumentation.
Indications:
Flexible, non-problematic curves;
Well-compensated deformities where function and pain are not severely compromised;
Elderly or frail patients where risks of aggressive correction outweigh benefits.
Method:
Fusion and decompression
Benefits:
Lower surgical morbidity
Reduced risk for perioperative complications, often effective in halting progression and stabilizing symptoms in balanced and less severe deformities.
Risks:
Does not improve alignment, may not relieve pain if it is due to malalignment or imbalance.
Axial back pain might persist if caused by the deformity itself rather than instability or stenosis
Aebi's Insight: If the global spinal balance is already acceptable, and the primary complaint is instability or localized pain (not due to malalignment), in situ fusion is appropriate, sparing patients from unnecessary and risky realignment procedures.
Complication
Revision surgery 20-40%
Patient Characteristics & Surgical Complexity:
Patients often have multiple pre-existing health conditions (comorbidities).
Operations are generally more involved, focusing on achieving proper balance and load sharing on surgical instrumentation.
Achieving correct load sharing is especially critical in patients with weakened bones (osteopenia).
Potential Local/Surgical Complications:
Infections
CSF leaks (more common in revision surgeries)
Implant failures
Junctional kyphosis (abnormal spinal curvature near the surgery site)
Adjacent segment degeneration (wear and tear on spinal levels next to the surgery)
Pseudarthrosis (failure of bones to fuse properly)
Potential Systemic Complications:
Myocardial infarction (heart attack)
Pneumonia
Ileus (temporary paralysis of the bowel)
Urinary tract infections (UTIs)
Deep venous thrombosis (DVT or blood clots, usually in the legs)
Superior mesenteric artery (SMA) syndrome (a digestive condition)
Blindness (exceedingly rare).
Overall Risk & Outcome Context:
Even with optimal techniques and post-operative care, complication rates can be somewhat high.
Despite the risks, the potential for positive clinical outcomes is considered sufficient to justify the procedures in appropriately selected patients.
 Made with Bullet
Made with Bullet