Numbers
- 0.3% of intracranial tumours
Location
- Have a tendency to occur near the midline
- Anterior fontanelle extradurally, and in the sellar, parasellar, and intraventricular regions intradurally.
- Most common intraspinal site is near the cauda equina, and can be associated with a dermal sinus tract and subsequent increased risk of bacterial infection.
Pathology
- Macroscopically
- Well- defined, lobulated, pearly masses with thick partially calcified capsules.
- Microscopically
- Exhibit both dermal and epidermal elements, although the epithelial cell lining may be less well differentiated compared with epidermoid cysts.
- Cyst contents: yellow, odious fluid that results from glandular secretion,
- Epithelial cell debris and keratin, and also include elements of dermis such as hair follicles, sebaceous glands and sweat glands
- Active secretion of glandular fluid and subsequent growth and rupture is postulated as a possible cause for their earlier presentation
- And may also contain hair and teeth.
Clinical presentation
- Insidious onset
- Due to Local mass effect
- Depends on tumour location
- Due to the slow, linear growth rate.
- Cysts in the middle cranial fossa are often asymptomatic,
- Can grow relatively large before detection,
- Atypical presentations such as trigeminal numbness.
- More acute presentation,
- Due to cyst rupture (traumatic, iatrogenic, or spontaneous) → leakage of cyst contents into the sub-arachnoid space → associated chemical meningitis.
- This should be distinguished from the septic meningitis (intraspinal dermoid cysts, caused by the presence of a dermal sinus tract)
- Cyst rupture can cause
- Headache, seizures, vasospasm, neurological deficit, and death.
- Association with other congenital abnormalities that may account for the initial presentation.
- Klippel- Feil syndrome has been reported for both intraspinal and intracranial dermoid cysts.
- The presence of associated mesenchymal abnormalities supports the notion put forward by Dias and Walker that the key embryological event for the development of dermoid cysts occurs prior to neural tube closure, around the time of the formation of the trilaminar plate
- All patients should be examined for signs of a dermal sinus tract, which may predispose to bacterial infection. In these cases, excision of the tract should be incorporated with the surgical resection of the cyst
Imaging
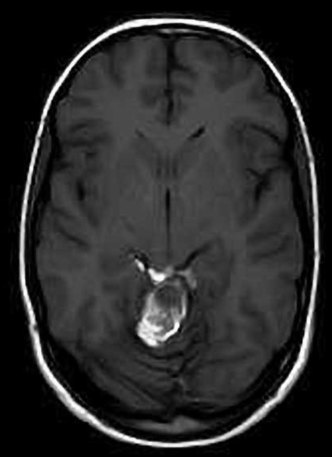
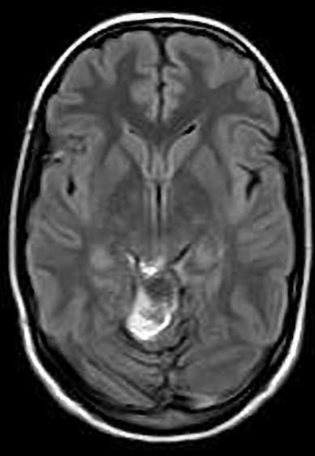
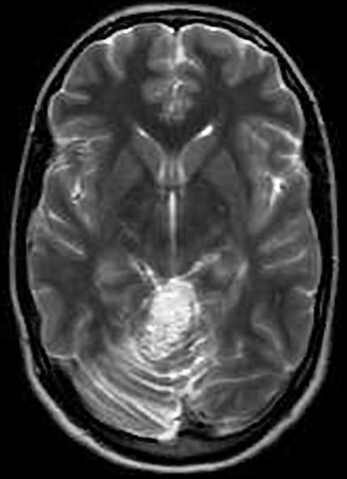
- Variable appearance on MRI, dependent on the balance of their contents which may include fat, hair, sebum, and teeth.
- They differ from lipomas by not consistently following fat densities on all sequences.
- Haemorrhage within the cyst can lead to hyperdensity on CT, and can occasionally mask the underlying lesion
Images

Management
General
- Corticosteroids are indicated following cyst rupture or postoperatively when cyst contents are spilled, when they are thought to reduce the severity and duration of chemical meningitis.
- No role for radiotherapy or chemotherapy in the treatment of dermoid or epidermoid cysts with the exception of malignant transformation.
Conservative
- Annual radiological (MRI) and clinical monitoring
Surgery
- Indication
- Diagnostic: Rarely needed because MRI is diagnostic most of the time
- Treatment of symptoms: usually secondary to the mass effect.
- Improvement in out-come: hard to predict what is natural history
- Goal of surgery is complete resection of the cyst including the epithelial lining
- Total resection: defined as complete removal of cyst contents and capsule
- Technical difficulties of surgery
- Deep
- Tumour adhesions to adjacent structures on the skull base and also to surrounding brain parenchyma are common.
- Dermoid cyst cause a greater granulomatous reaction with the arachnoid mater and occasionally the pia mater.
- The cyst can extend between different anatomical compartments
- More often in epidermoid cysts, which are soft and pliable and have a tendency to ‘flow’ into the available subarachnoid space.
- Prolonged linear growth of tumours can lead to substantial distortion of the surrounding anatomy, such as dis-placement of the basilar artery from the ventral surface of the brain-stem.
- Dermoid cysts may present more of a challenge in the development of a plane between capsule and arachnoid in areas of granulomatous reaction, while epidermoid cysts may be more challenging in their anatomical lo-cation and extension
- Complication
- Spilling’ of the contents of the cyst into the surrounding CSF
- Which can occur with intraoperative handling in both epidermoid and dermoid cyst.
- Dissemination of fat droplets throughout the subarachnoid and intraventricular space, setting up a chemical inflammation of the meninges
- Clinical sequelae are variable, and include no adverse effects, headaches, seizures, and hydrocephalus
- Risk of intraoperative spillage can be reduced by sharp dissection of the capsule, copious irrigation in the surgical field and protection of the surrounding brain with cotton pads.
- Treatment is largely conservative, although steroids are indicated for chemical meningitis, and hydrocephalus should be treated with appropriate CSF diversion.
- Recurrence
- Dependent on the volume of residual tumour left following subtotal resection
 Made with Bullet
Made with Bullet