Location
- Petrosal surface
- Unilateral
- Cerebellar lobules that wrap around to the anterior surface:
- Quadrangular
- Simple
- Superior semilunar
- Inferior semilunar
- Biventral lobules.
- They are distinct from lateral pontine AVMs that are based in the lateral pons and middle cerebellar peduncle.
- Petrosal AVMs are cerebellar rather than pontine, and therefore reside lateral to CN7/8.
Arterial supply
- Cortical branches of the AICA.
Venous drainage
- Anterior Hemispheric Vein
- Vein of cerebellar pontine fissure
- Which then course to
- Superior petrosal vein (SPetrV)
- Superior petrosal sinus (SPS)
Non-eloquent
- But not far from CN5, CN7/8, and pons.
Resection strategy
- Approach
- Extended retrosigmoid approach (step 1)
- Skeletonizes SigmS from the transversesigmoid junction to the jugular bulb
- Dural flap
- So the sinus can be pulled anteriorly
- Maximize the opening into the cerebellopontine angle
- Minimizes the need for fixed retraction
- Arachnoid dissection
- Step 2, approaching the AVM through the cerebellopontine cistern;
- Subarachnoid dissection opens the arachnoid of the brainstem cisterns, (Step 2)
- CbPonC
- PonC
- CbMedC
- MedC
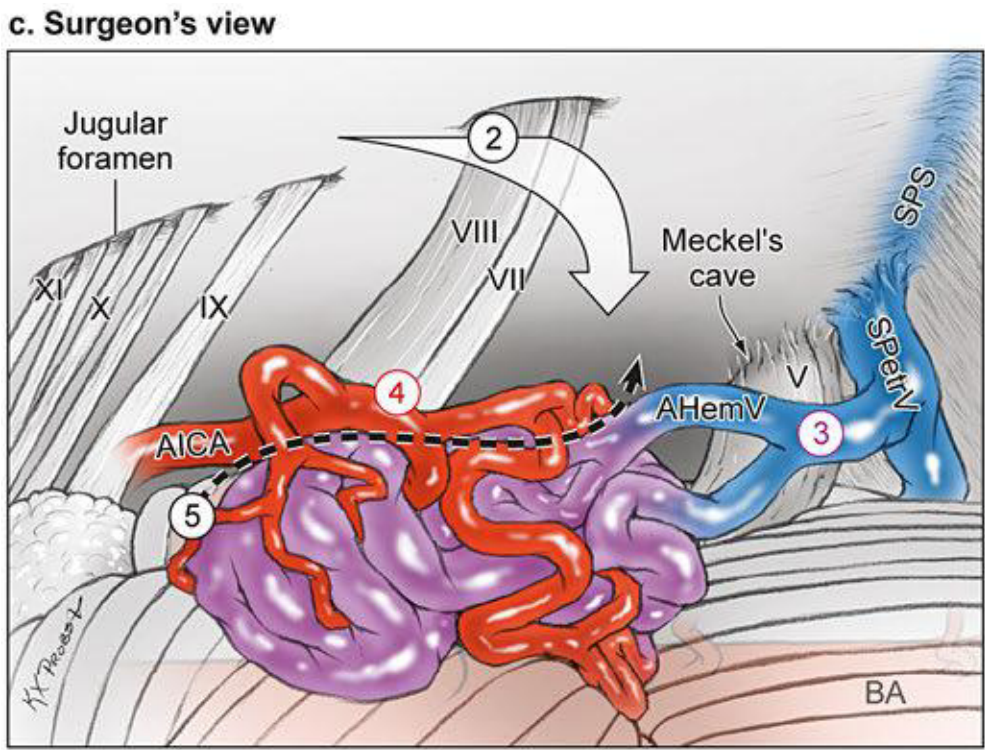
- Step 3, identifying the draining veins ascending medially;
- The AVM drainage is deep via AHemV and VCPonF, which course to SPetrV (Dandy’s vein) and SPS
- Step 4, locating the AICA feeders lateral to CN7/8;
- The AICA feeders arise from the a3 and a4 segments (step 4)
- Step 5, interrupting the medial front near the flocculus
- Feeder are interrupted early by advancing medial to the nidus (step 5).
- However, many of these medial feeders cannot be visualized early in the resection, and their interruption must wait until the deep dissection.
- Dissection is centred around
- CN7/8 and the AICA
- Extends
- Superiorly to CN5 when the SCA contributes to the AVM
- Inferiorly to CN9/10/11 when the PICA contributes.
- The approach trajectory is perpendicular rather than parallel, which means that the lateral and posterior AVM margins are accessed at the expense of some overlying cerebellum.
- An incision in the cerebellar cortex is made lateral to the AVM and some intervening lobule is resected to reach the lateral AVM margin and open a seam to the medial side.
- With ruptured AVMs, hemispheric hematomas may have already opened this seam, and early evacuation accesses the medial side while also relaxing swollen cerebellum.
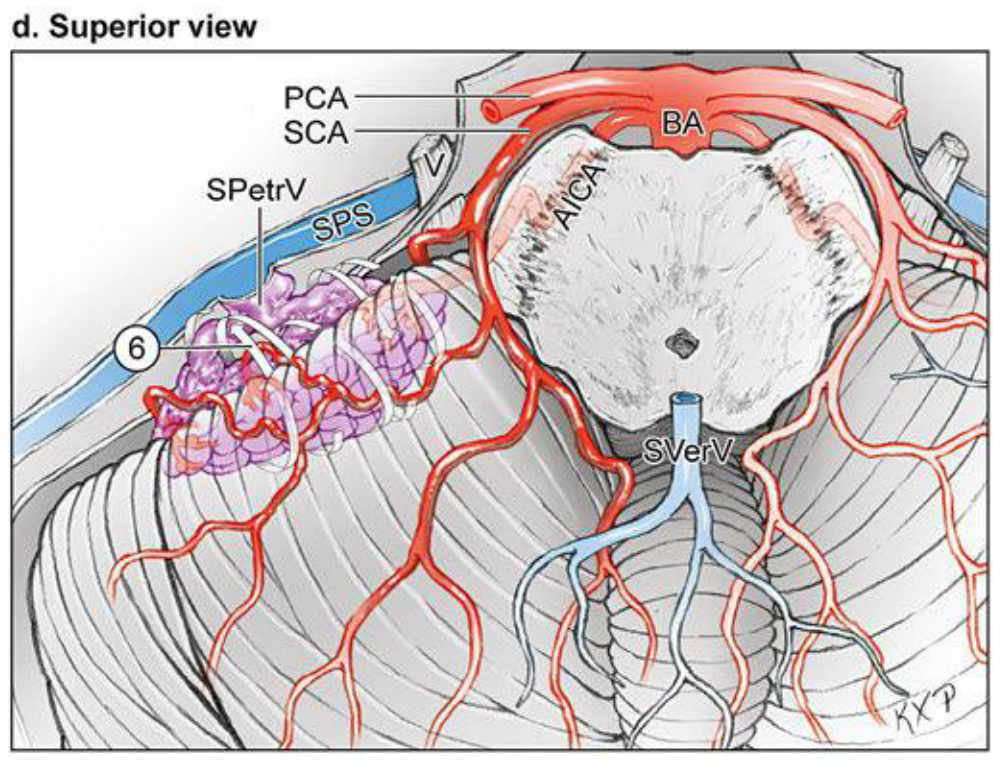
- Step 6, circumdissecting the lateral, superior, and inferior margins in the cerebellum (“back door” technique, superior view of the cerebellum).
- The AVM is then circumscribed, dissecting around the back side and rolling it anteriorly away from the middle cerebellar peduncle and cranial nerves deep to the nidus (step 6)
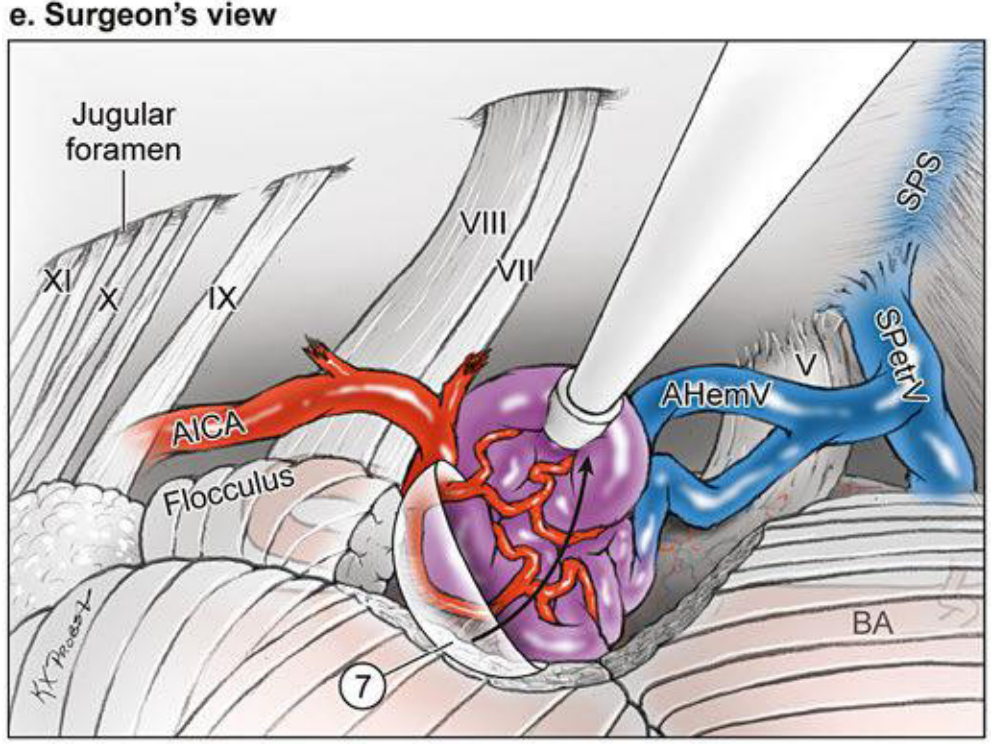
- Step 7, mobilizing the AVM anteriorly to dissect the posterior and medial planes and divide the medial AICA feeders (surgeon’s view).
- Scooping the AVM from behind leaves deep medial feeders until the end of the dissection and also preserves the attachment of the draining vein to SPS (step 7).
- Petrosal AVMs are non-eloquent but adjacent to pons, middle cerebellar peduncle, and CN7/8.
- The dissection lateral to the cranial nerves avoids entry into the brainstem.
 Made with Bullet
Made with Bullet